
Neonatal Pulmonology - Basic/Translational Science 3
Session: Neonatal Pulmonology - Basic/Translational Science 3
 photo")
Morarji Peesay (he/him/his)
Associate Professor
Georgetown University Hospital
Washington DC, District of Columbia, United States
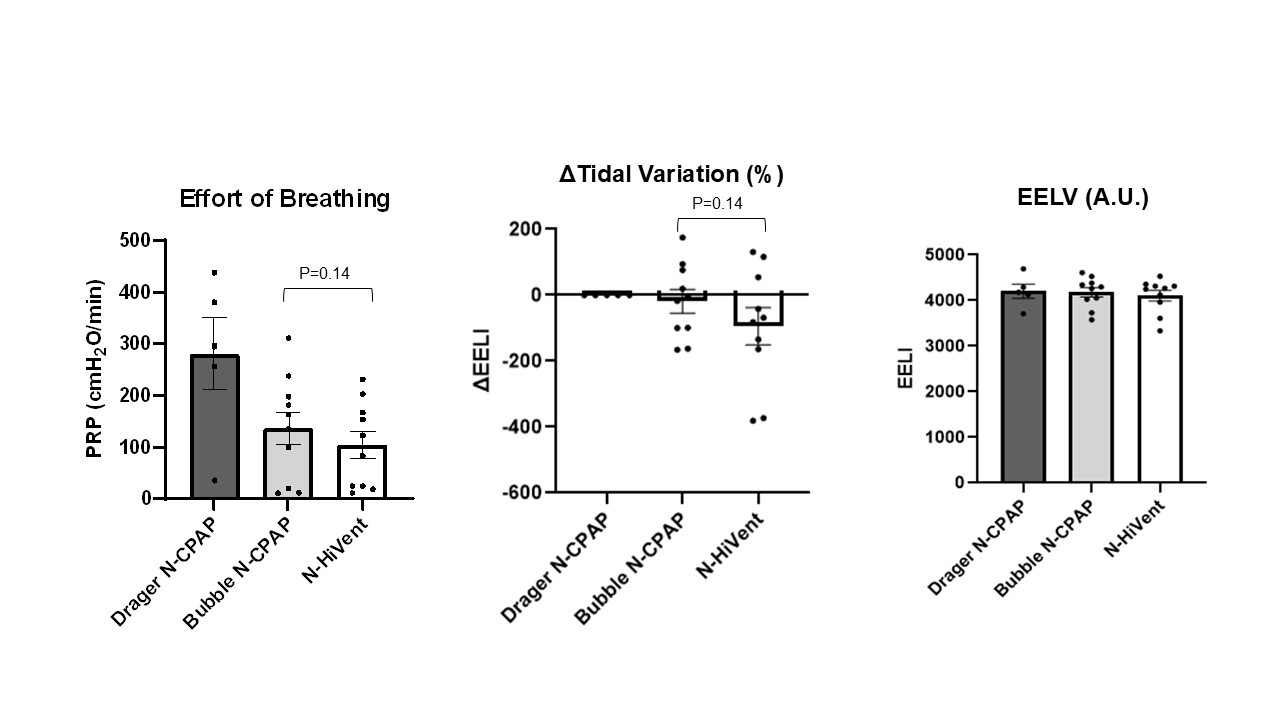 There is no difference in Tidal Variation among three devices. HiVent device change in EELI values hover around zero with minor variations - stability of lung volumes similar to Bubble CPAP. All three devices show similar EELV values around 4000 A.U. EELI (End Expiratory Lung Impedance) represents changes in lung volumes
There is no difference in Tidal Variation among three devices. HiVent device change in EELI values hover around zero with minor variations - stability of lung volumes similar to Bubble CPAP. All three devices show similar EELV values around 4000 A.U. EELI (End Expiratory Lung Impedance) represents changes in lung volumes.jpg) No significant difference between devices
No significant difference between devices