
Emergency Medicine 11
Session: Emergency Medicine 11
 Credit")
 photo")
Sarika K. Sheth, MD (she/her/hers)
Assistant Clinical Professor
Rady Children's Hospital San Diego
San Diego, California, United States
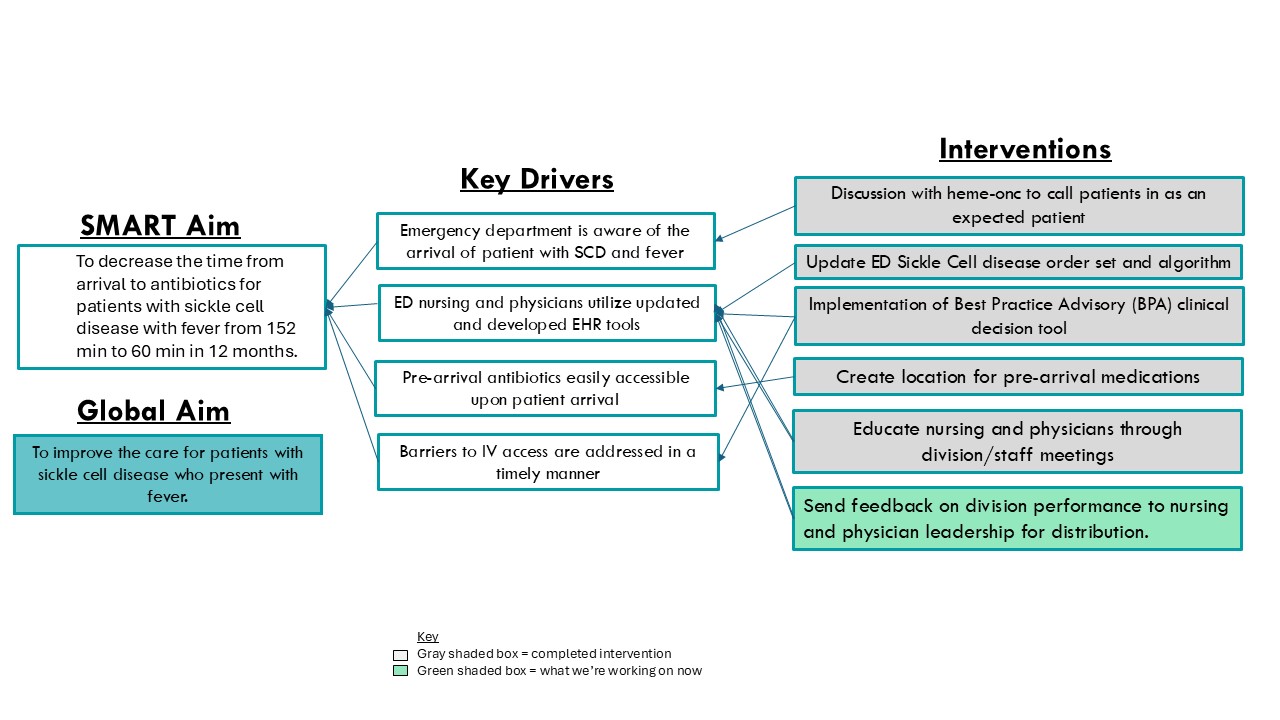 Key Driver Diagram
Key Driver Diagram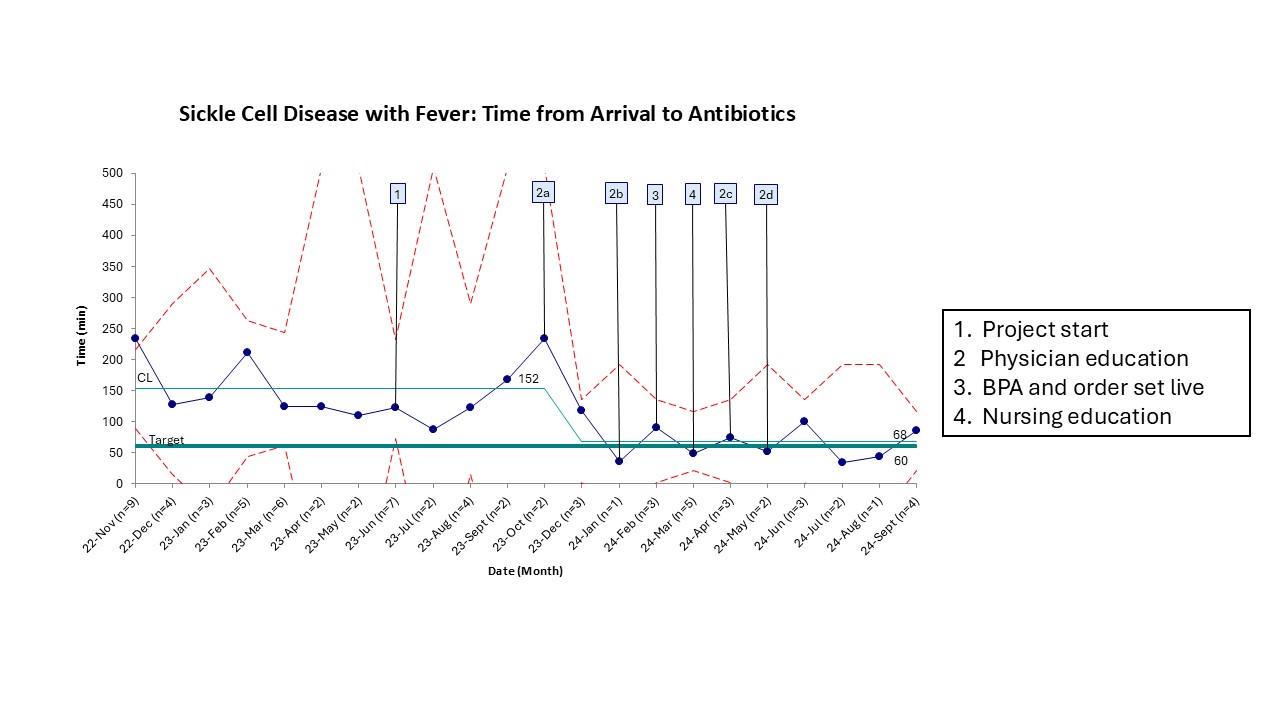 Sickle Cell Disease with Fever: Time from Arrival to Antibiotics
Sickle Cell Disease with Fever: Time from Arrival to Antibiotics.jpg) Sickle Cell Disease with Fever: Time from Room to Antibiotics
Sickle Cell Disease with Fever: Time from Room to Antibiotics