
Emergency Medicine 13
Session: Emergency Medicine 13
 photo")
Jennifer Hockenbury, MD (she/her/hers)
Pediatric Emergency Medicine Fellow
University of Louisville School of Medicine
Louisville, Kentucky, United States
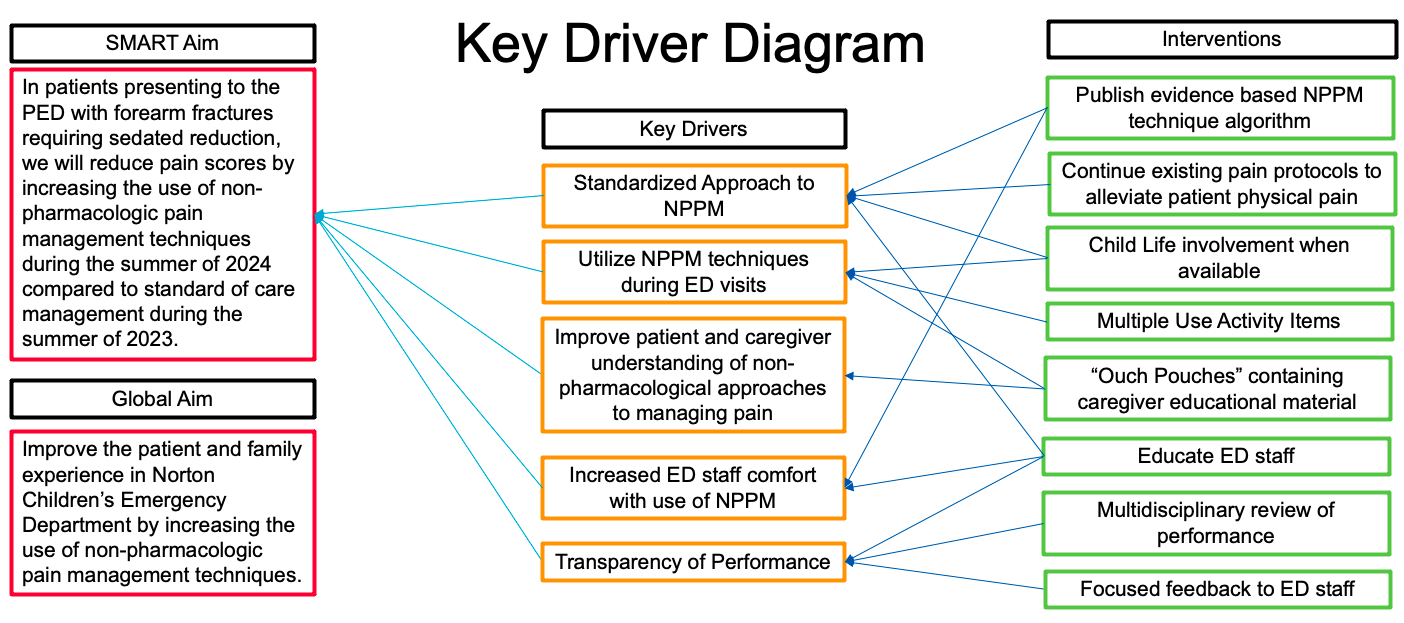 Study Design Key Driver Diagram.
Study Design Key Driver Diagram..png) Non-Pharmacologic Pain Management Algorithm.
Non-Pharmacologic Pain Management Algorithm..jpg) Multivariate binomial regression predicting if a subject found improvement in their FLACC score.Study Design Key Driver Diagram.Non-Pharmacologic Pain Management Algorithm.Multivariate binomial regression predicting if a subject found improvement in their FLACC score.
Multivariate binomial regression predicting if a subject found improvement in their FLACC score.Study Design Key Driver Diagram.Non-Pharmacologic Pain Management Algorithm.Multivariate binomial regression predicting if a subject found improvement in their FLACC score.