
Neonatal GI Physiology & NEC 3
Session: Neonatal GI Physiology & NEC 3

Michelle Hojnicki, DO
Neonatologist
Johns Hopkins All Children's Hospital - 501 6th Ave SSt. Petersburg, FL 33701UNITED STATES - St. Pe
Palmetto, Florida, United States
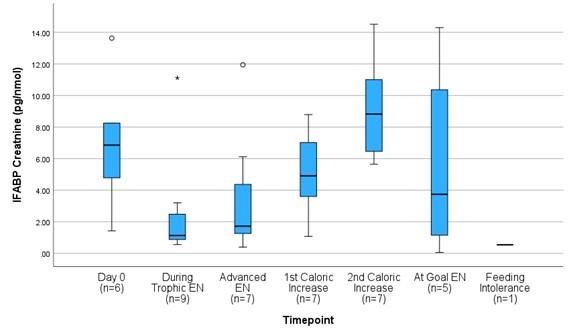 Urinary intestinal fatty-acid binding protein (I-FABP) corrected to urine creatinine (pg/nmol) levels of preterm infants 25-31 weeks gestational age from the initiation through full provision of enteral nutrition (EN.)
Urinary intestinal fatty-acid binding protein (I-FABP) corrected to urine creatinine (pg/nmol) levels of preterm infants 25-31 weeks gestational age from the initiation through full provision of enteral nutrition (EN.)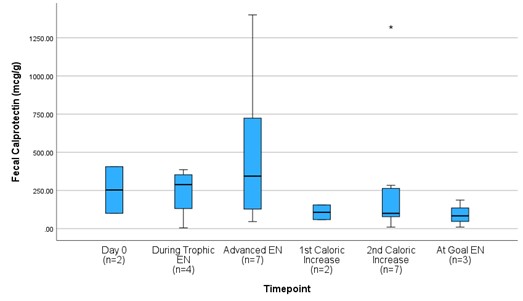 Fecal calprotectin (fCal) (mcg/g) levels of preterm infants 25-31 weeks gestational age from the initiation through full provision of enteral nutrition (EN.)
Fecal calprotectin (fCal) (mcg/g) levels of preterm infants 25-31 weeks gestational age from the initiation through full provision of enteral nutrition (EN.)