
Neonatal GI Physiology & NEC 4
Session: Neonatal GI Physiology & NEC 4
Katie Huff, MD, MS (she/her/hers)
Assistant Professor of Clinical Pediatrics
Indiana University School of Medicine
Indianapolis, Indiana, United States
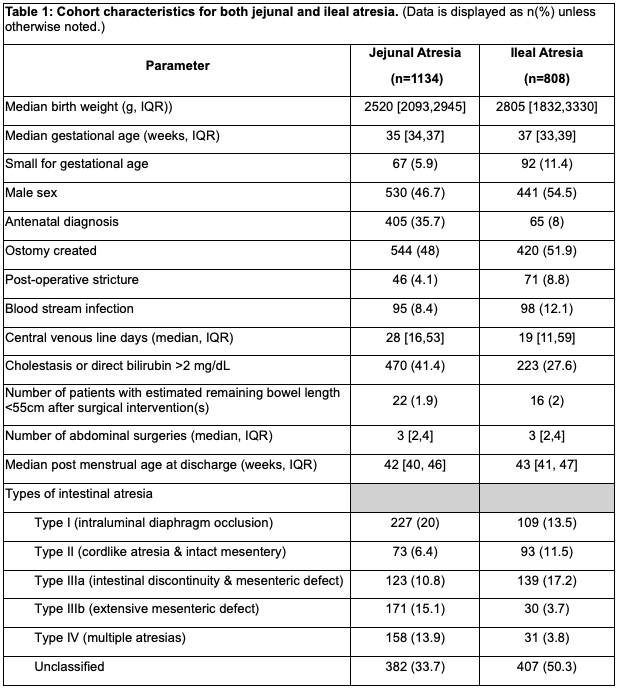 (Data is displayed as n(%) unless otherwise noted.)
(Data is displayed as n(%) unless otherwise noted.)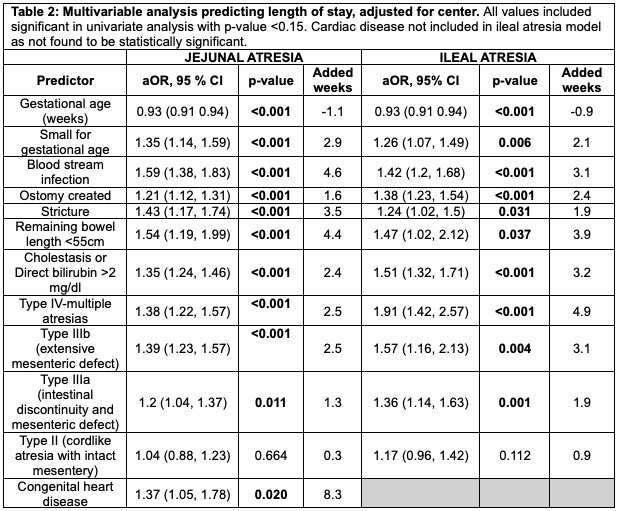 All values included significant in univariate analysis with p-value <0.15. Cardiac disease not included in ileal atresia model as not found to be statistically significant.
All values included significant in univariate analysis with p-value <0.15. Cardiac disease not included in ileal atresia model as not found to be statistically significant.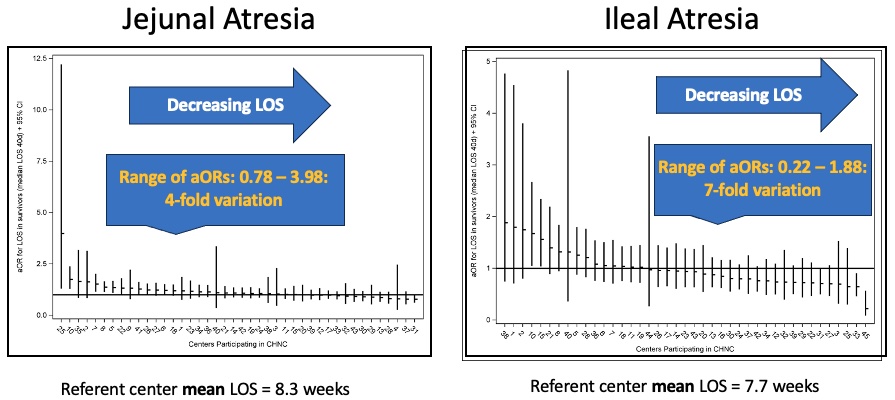 Each line represents an individual center adjusted odds ratio and 95% confidence interval. Blinded center codes represent the same hospital on each graph panel. After adjusting for the variables in Table 2, risk-adjusted LOS demonstrated striking variations between hospitals (JA: 6.6 to 33 weeks; IA: 1.7 to 14.5; p<0.001 for both).
Each line represents an individual center adjusted odds ratio and 95% confidence interval. Blinded center codes represent the same hospital on each graph panel. After adjusting for the variables in Table 2, risk-adjusted LOS demonstrated striking variations between hospitals (JA: 6.6 to 33 weeks; IA: 1.7 to 14.5; p<0.001 for both).