
Neonatal Fetal Nutrition & Metabolism 4
Session: Neonatal Fetal Nutrition & Metabolism 4
 photo")
Margaret L. Ong, MD, MPH (she/her/hers)
Neonatologist
Brigham and Women's Hospital
Boston, Massachusetts, United States
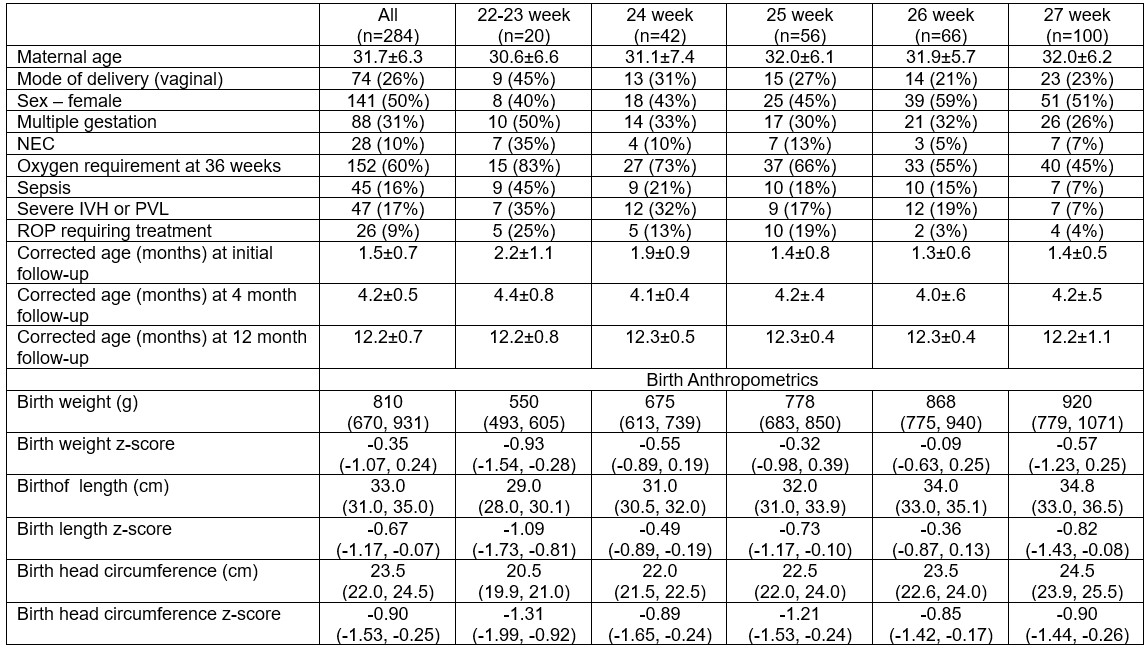 Demographic data are represented as mean±SD or n (% of gestational age category n). Anthropometric z-scores are presented as median (IQR). NEC: necrotizing enterocolitis. Sepsis: early/late onset bacterial or fungal sepsis. Severe IVH or PVL: grade III-IV intraventricular hemorrhage or periventricular leukomalacia. ROP: retinopathy of prematurity. Birth z-scores were derived using Olsen reference. Note: birth anthropometric z-scores for 22-23 week group do not capture <23 week on Olsen reference.
Demographic data are represented as mean±SD or n (% of gestational age category n). Anthropometric z-scores are presented as median (IQR). NEC: necrotizing enterocolitis. Sepsis: early/late onset bacterial or fungal sepsis. Severe IVH or PVL: grade III-IV intraventricular hemorrhage or periventricular leukomalacia. ROP: retinopathy of prematurity. Birth z-scores were derived using Olsen reference. Note: birth anthropometric z-scores for 22-23 week group do not capture <23 week on Olsen reference. 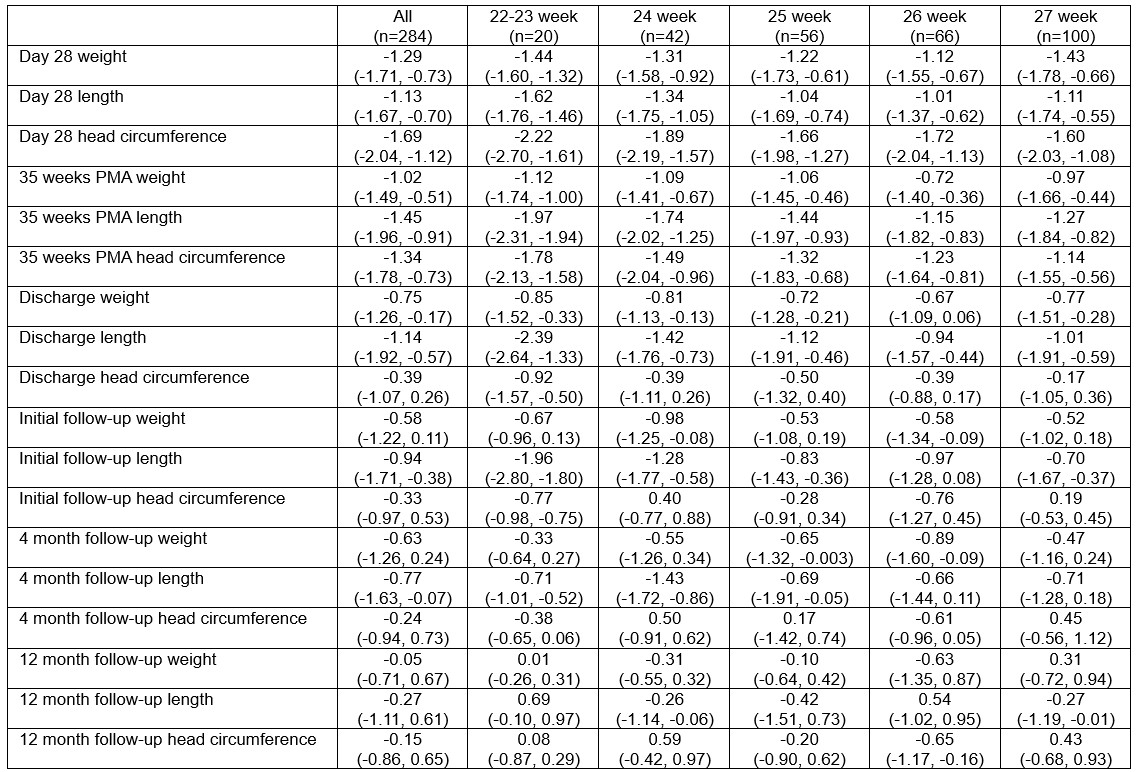 Data are represented as median (IQR). Z-scores were derived using Olsen reference for PMA ≤41 week and WHO reference (for corrected age) for PMA >41 weeks.
Data are represented as median (IQR). Z-scores were derived using Olsen reference for PMA ≤41 week and WHO reference (for corrected age) for PMA >41 weeks. 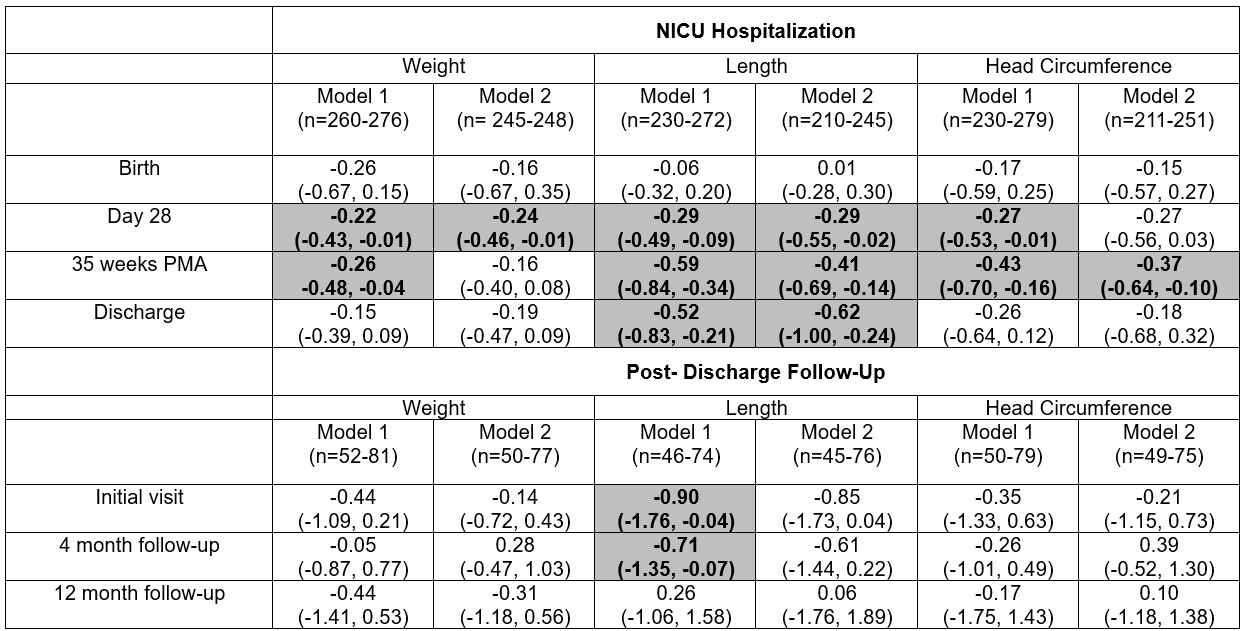 PMA: post-menstrual age. Beta estimates indicate difference in median anthropometric z-score comparing infants born ≤24 weeks gestation vs those born >24 weeks (reference). Median regression models were adjusted for covariates of interest. Model 1 adjusted for multiple gestation and size for GA at birth (small, average, or large for gestational age), except models for birth which do not adjust for birth size. Model 2 adjusted for covariates in Model 1 + comorbidity count as an indicator of clinical illness (oxygen requirement at 36 weeks, retinopathy of prematurity requiring treatment, and intraventricular hemorrhage grade III or IV or periventricular leukomalacia). Z-scores were calculated using Olsen reference for PMA ≤41 week and WHO reference (for corrected age) for PMA >41 weeks. Shaded bolded results indicate p<0.05. Note: birth anthropometric z-scores do not capture <23 week on Olsen reference.
PMA: post-menstrual age. Beta estimates indicate difference in median anthropometric z-score comparing infants born ≤24 weeks gestation vs those born >24 weeks (reference). Median regression models were adjusted for covariates of interest. Model 1 adjusted for multiple gestation and size for GA at birth (small, average, or large for gestational age), except models for birth which do not adjust for birth size. Model 2 adjusted for covariates in Model 1 + comorbidity count as an indicator of clinical illness (oxygen requirement at 36 weeks, retinopathy of prematurity requiring treatment, and intraventricular hemorrhage grade III or IV or periventricular leukomalacia). Z-scores were calculated using Olsen reference for PMA ≤41 week and WHO reference (for corrected age) for PMA >41 weeks. Shaded bolded results indicate p<0.05. Note: birth anthropometric z-scores do not capture <23 week on Olsen reference.