
Public Health & Prevention 4
Session: Public Health & Prevention 4
 photo")
Allison Watts, PhD (she/her/hers)
Project Manager
University of British Columbia Faculty of Medicine
Vancouver, British Columbia, Canada
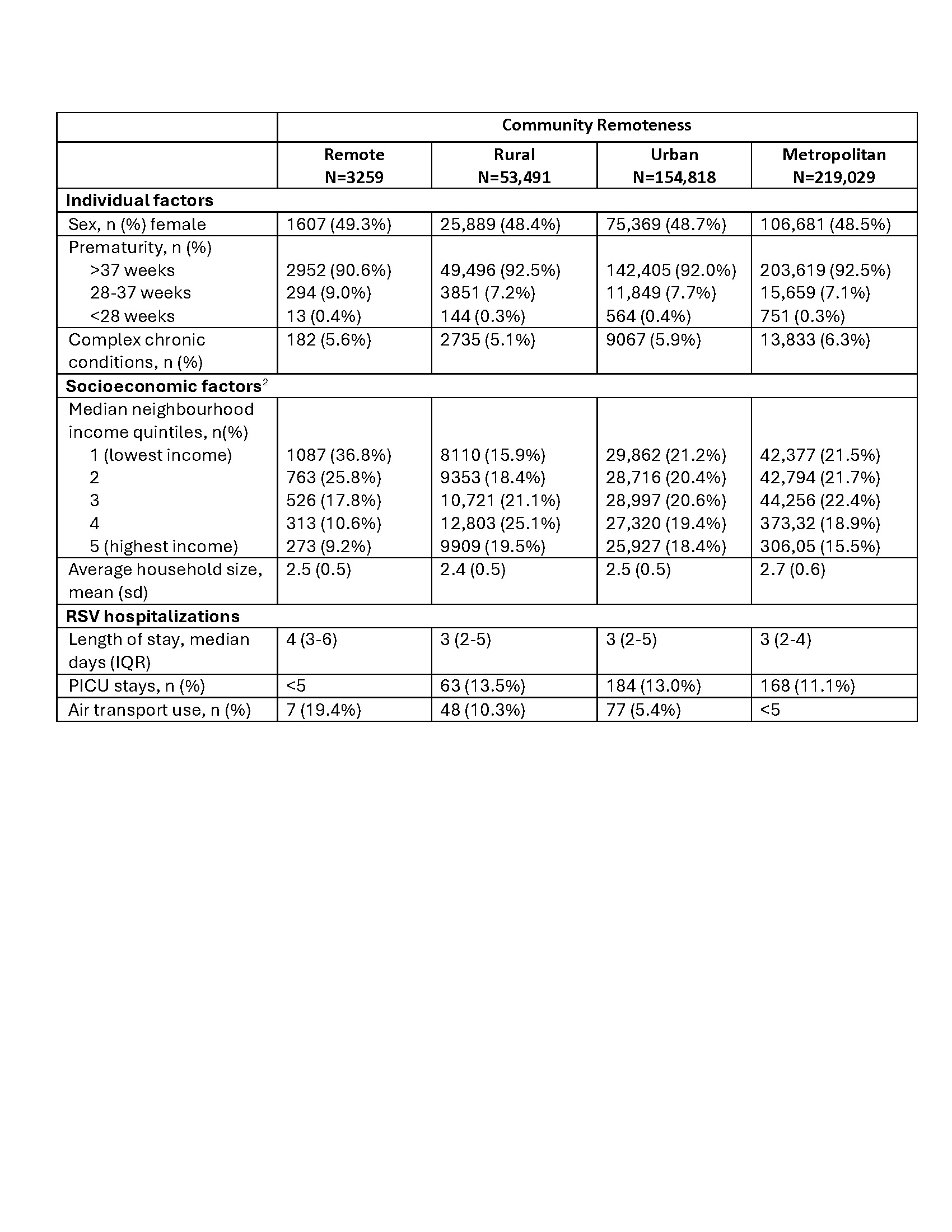 2-missing data on income and household size, respectively (n=40,286 [9.4%]; n=40,781 [9.5%] / 430,597)
2-missing data on income and household size, respectively (n=40,286 [9.4%]; n=40,781 [9.5%] / 430,597)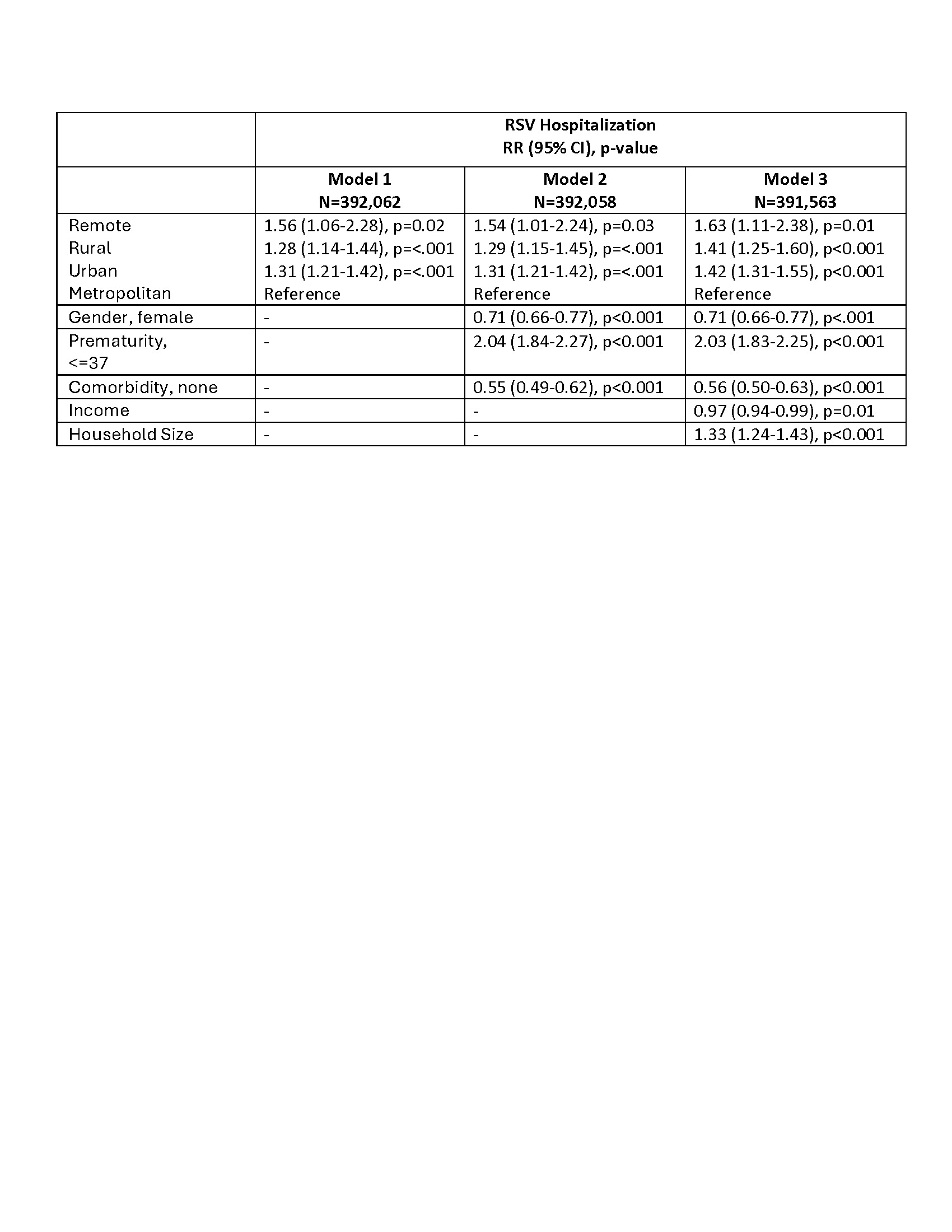 Mixed-effects Poisson regression accounting for clustering within communities
Mixed-effects Poisson regression accounting for clustering within communities