
Neonatal Hematology & Bilirubin Metabolism 2
Session: Neonatal Hematology & Bilirubin Metabolism 2

Ellen C. Ingolfsland, MD
Assistant Professor
University of Minnesota Medical School
Minneapolis, Minnesota, United States
.jpg) Association between iron status at 14, 28, and 42 days with ROP Stage ≥ 2, adjusted for potentially mediating variables. All logistic regression models adjusted for GA at birth, BW z-score, treatment group, site and a random effect for sibship. Reference is iron sufficient group.
Association between iron status at 14, 28, and 42 days with ROP Stage ≥ 2, adjusted for potentially mediating variables. All logistic regression models adjusted for GA at birth, BW z-score, treatment group, site and a random effect for sibship. Reference is iron sufficient group.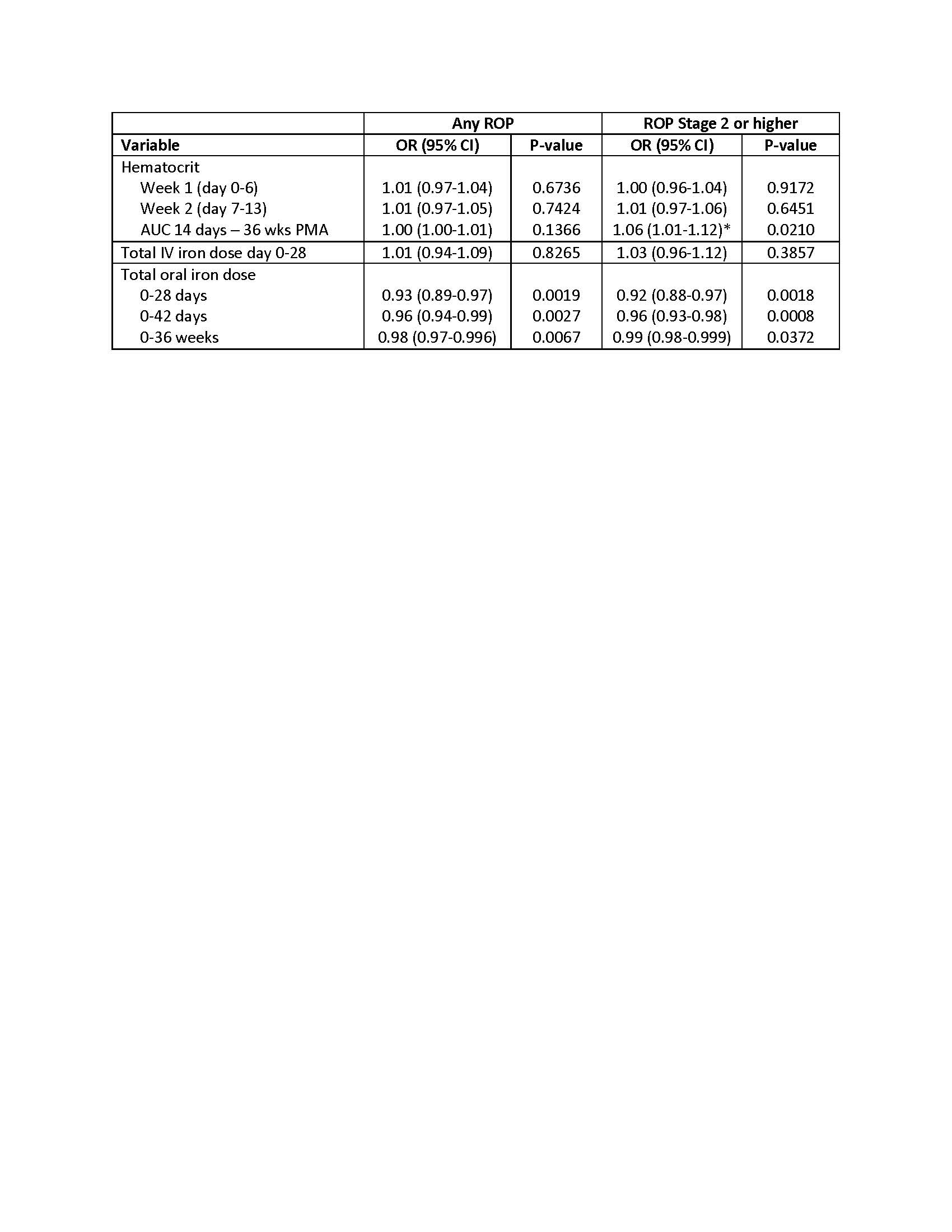 Logistic regression models of hematologic variables and ROP outcomes, adjusted for PMA at birth, birthweight z-score, treatment group, site and a random effect for sibship. Odds ratio is based on a change in 100 units for hematocrit and 10 units for oral iron dosing. Association between iron status at 14, 28, and 42 days with ROP Stage ≥ 2, adjusted for potentially mediating variables. All logistic regression models adjusted for GA at birth, BW z-score, treatment group, site and a random effect for sibship. Reference is iron sufficient group.Logistic regression models of hematologic variables and ROP outcomes, adjusted for PMA at birth, birthweight z-score, treatment group, site and a random effect for sibship. Odds ratio is based on a change in 100 units for hematocrit and 10 units for oral iron dosing.
Logistic regression models of hematologic variables and ROP outcomes, adjusted for PMA at birth, birthweight z-score, treatment group, site and a random effect for sibship. Odds ratio is based on a change in 100 units for hematocrit and 10 units for oral iron dosing. Association between iron status at 14, 28, and 42 days with ROP Stage ≥ 2, adjusted for potentially mediating variables. All logistic regression models adjusted for GA at birth, BW z-score, treatment group, site and a random effect for sibship. Reference is iron sufficient group.Logistic regression models of hematologic variables and ROP outcomes, adjusted for PMA at birth, birthweight z-score, treatment group, site and a random effect for sibship. Odds ratio is based on a change in 100 units for hematocrit and 10 units for oral iron dosing. 