
Neonatal/Infant Resuscitation 3
Session: Neonatal/Infant Resuscitation 3
.jpeg.jpg "Vivek Shukla, MD photo")
Vivek Shukla, MD
Assistant Professor
University of Alabama at Birmingham
Birmingham, Alabama, United States
.png)
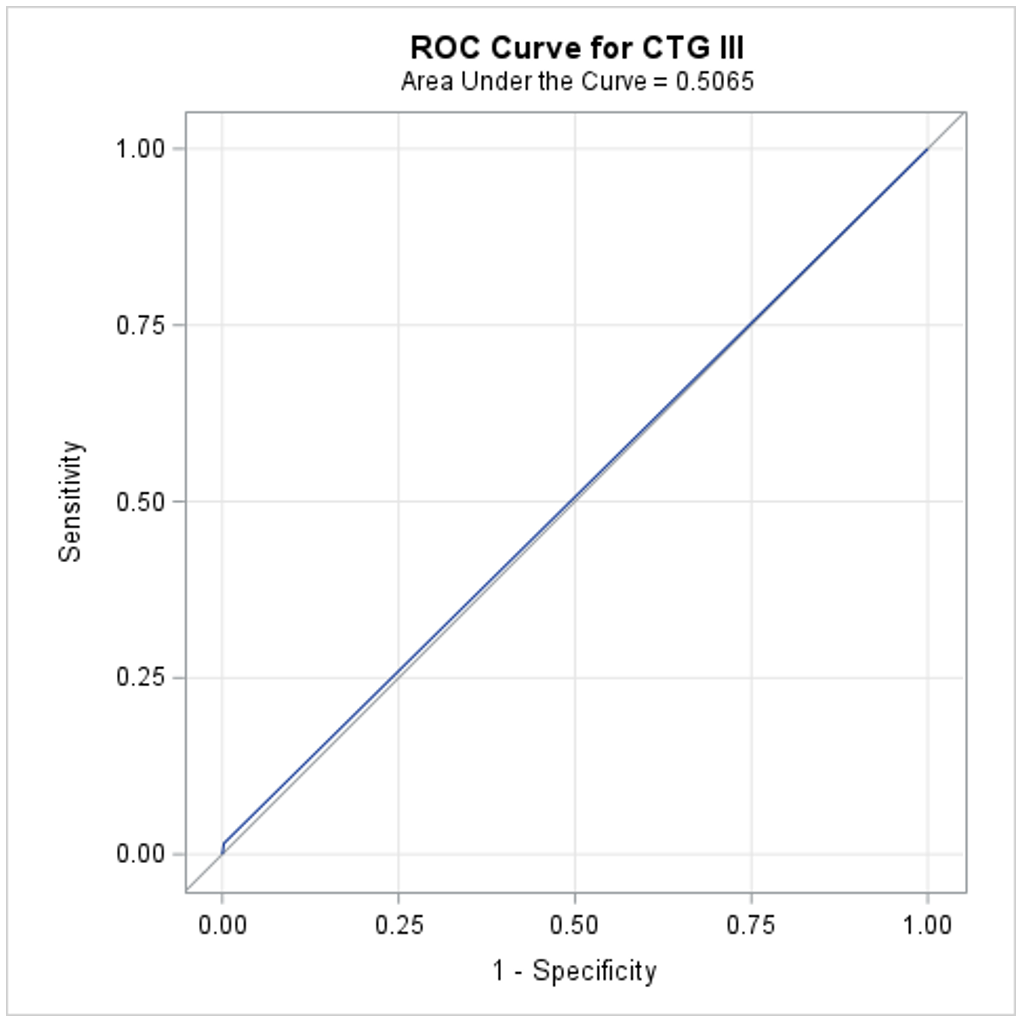 AUC = 0.506, sensitivity = 0.015, specificity = 0.997, PPV = 0.085, NPV = 0.986, indicating the inadequacy of current CTG categorization for predicting perinatal depression.
AUC = 0.506, sensitivity = 0.015, specificity = 0.997, PPV = 0.085, NPV = 0.986, indicating the inadequacy of current CTG categorization for predicting perinatal depression.