
Neonatal/Infant Resuscitation 4
Session: Neonatal/Infant Resuscitation 4
Marta Thio, Doctor
Neonatal Consultant
The Royal Women's Hospital Melbourne
Albert Park, Victoria, Australia
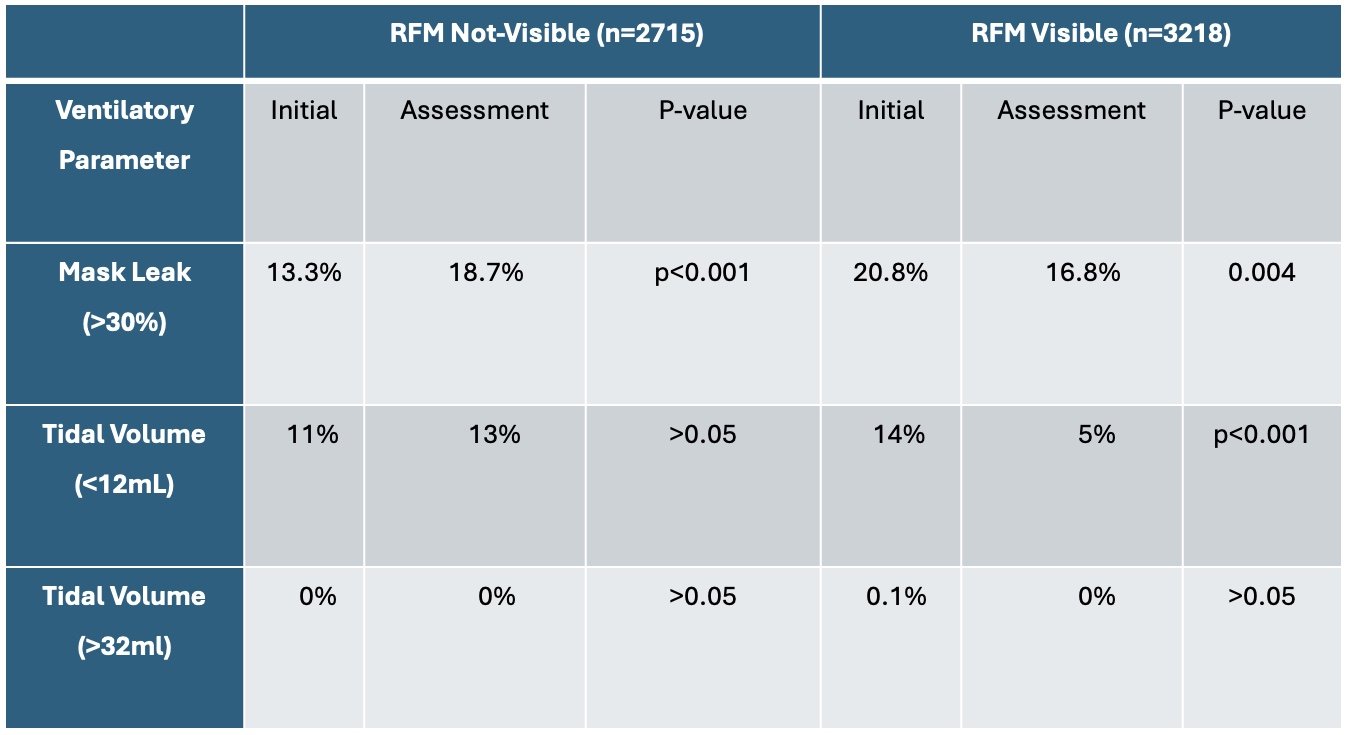 Proportion of inflations outside of the target range for mask leak and tidal volume. RFM; respiratory function monitor
Proportion of inflations outside of the target range for mask leak and tidal volume. RFM; respiratory function monitor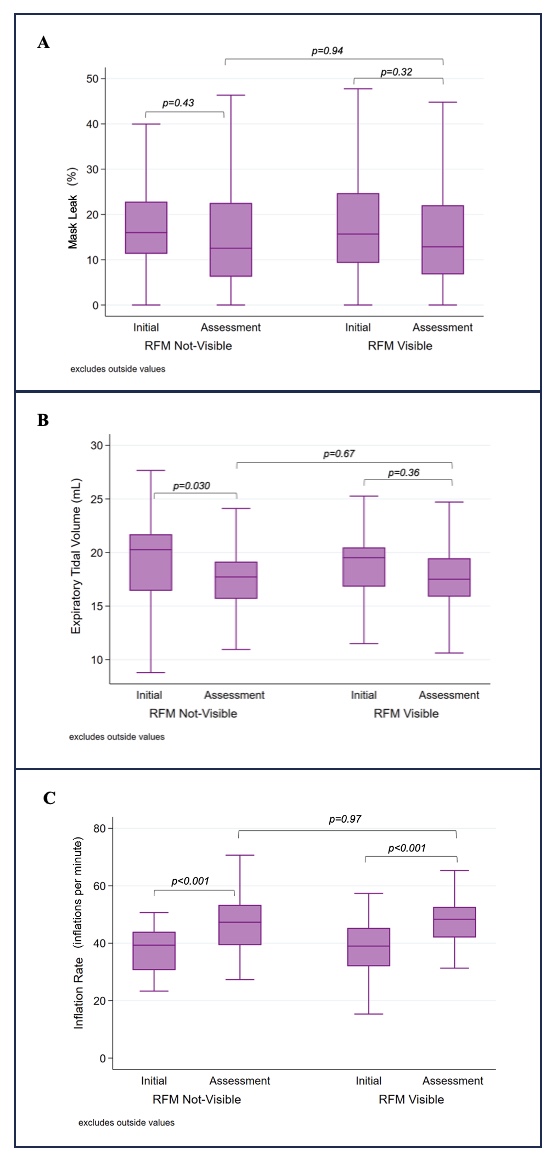 Mask leak (A), expiratory tidal volume (B), inflation rate (C) during 90 seconds of face-mask ventilation for both an initial and assessment session, according to respiratory function monitor (RFM) training group (n=49). The median is represented by the horizontal line in the centre of the box, the interquartile range is shown through the upper and lower boundaries of the box and the whiskers demonstrate the range. A paired t-test and unpaired t-test were performed. P-values are shown on the graphs ( <0.05 statistically significant).
Mask leak (A), expiratory tidal volume (B), inflation rate (C) during 90 seconds of face-mask ventilation for both an initial and assessment session, according to respiratory function monitor (RFM) training group (n=49). The median is represented by the horizontal line in the centre of the box, the interquartile range is shown through the upper and lower boundaries of the box and the whiskers demonstrate the range. A paired t-test and unpaired t-test were performed. P-values are shown on the graphs ( <0.05 statistically significant).