
Neonatal/Infant Resuscitation 3
Session: Neonatal/Infant Resuscitation 3
 photo")
Nicholas Plachinski, DO (he/him/his)
Resident
Medical College of Wisconsin
Cedarburg, Wisconsin, United States
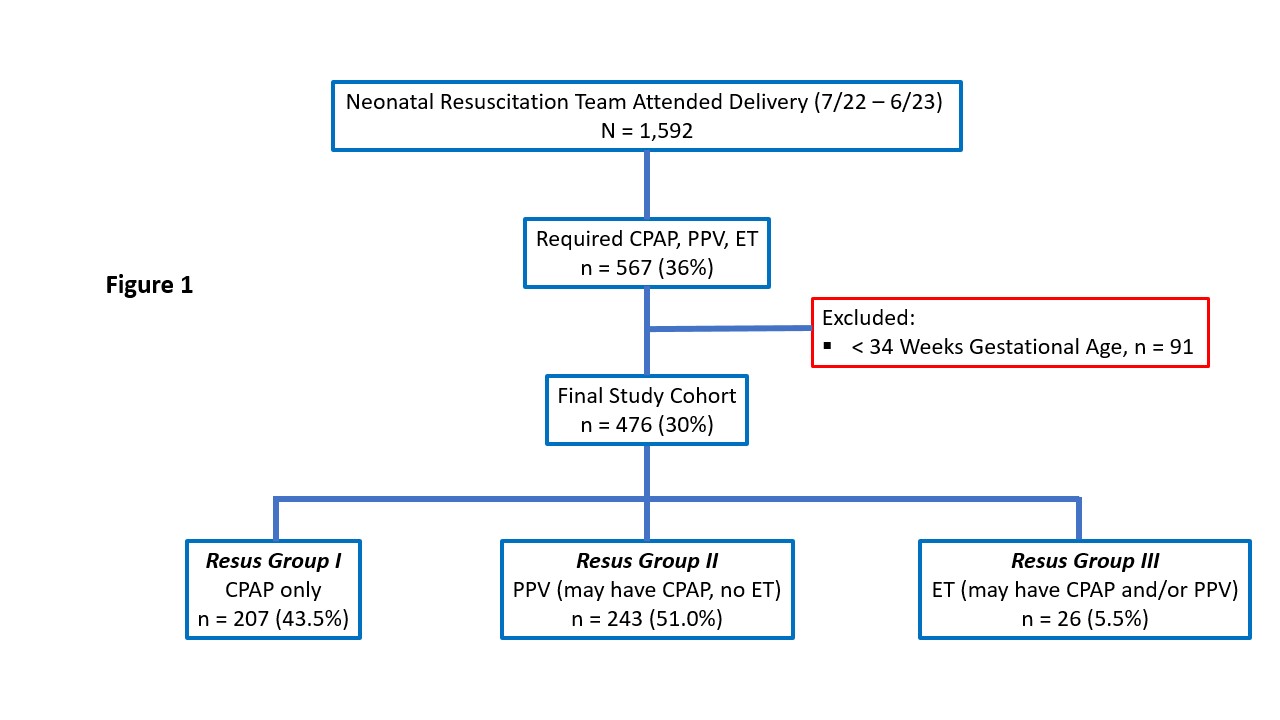 Flow diagram showing the selection process starting with delivery room resuscitation, and to three groups CPAP only, PPV (may have CPAP, no ET), ET (may have CPAP and/or PPV).
Flow diagram showing the selection process starting with delivery room resuscitation, and to three groups CPAP only, PPV (may have CPAP, no ET), ET (may have CPAP and/or PPV)..jpg) Table 1A: comparison of maternal demographics and risk factors between the three groups
Table 1A: comparison of maternal demographics and risk factors between the three groups.jpg) Figure 2A: comparison of CPAP duration between resus group 1 and resus group 2&3.
Figure 2A: comparison of CPAP duration between resus group 1 and resus group 2&3.