
Neonatal/Infant Resuscitation 3
Session: Neonatal/Infant Resuscitation 3
 photo")
Nicholas Plachinski, DO (he/him/his)
Resident
Medical College of Wisconsin
Cedarburg, Wisconsin, United States
.jpg) Flow diagram showing the selection process starting with initial resuscitation to those with placental specimens, and to two groups [ < 34 weeks (PT) vs. ≥ 34 weeks (LPT/T)]
Flow diagram showing the selection process starting with initial resuscitation to those with placental specimens, and to two groups [ < 34 weeks (PT) vs. ≥ 34 weeks (LPT/T)]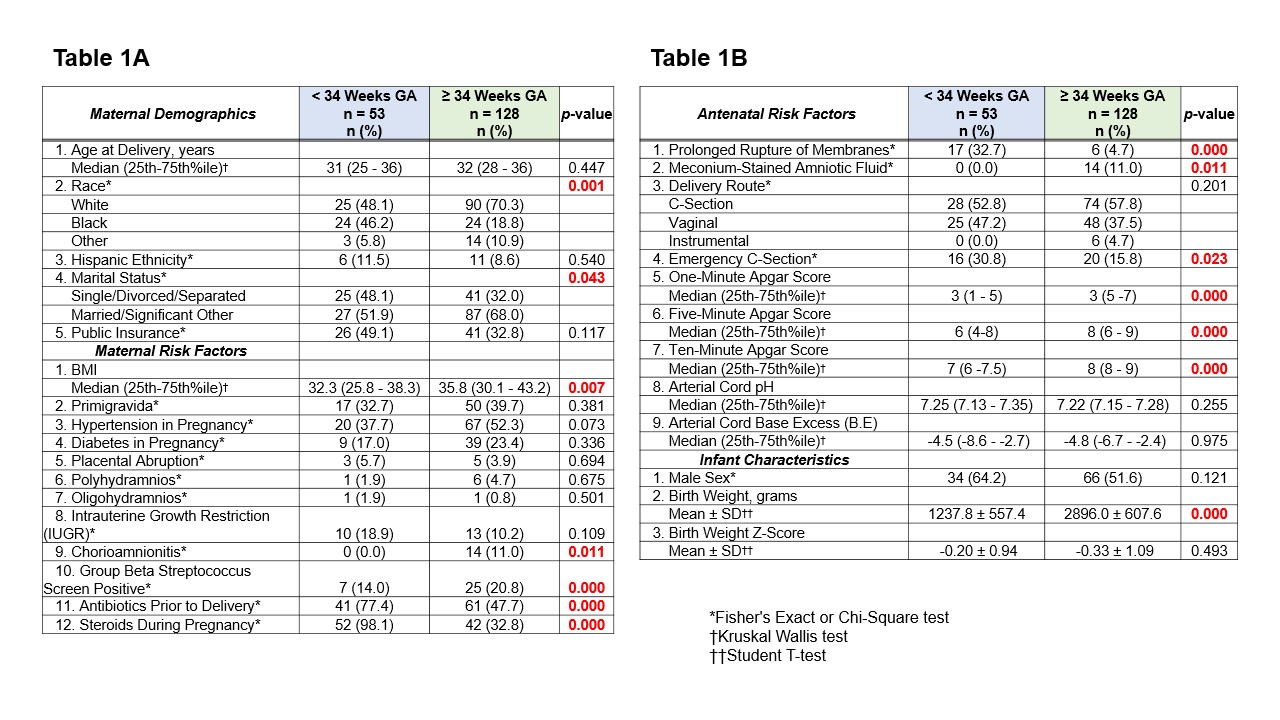 Table 1A . Comparison of maternal demographics and risk factors between the two groups [ < 34 weeks (PT) vs. ≥ 34 weeks (LPT/T)].
Table 1A . Comparison of maternal demographics and risk factors between the two groups [ < 34 weeks (PT) vs. ≥ 34 weeks (LPT/T)]. 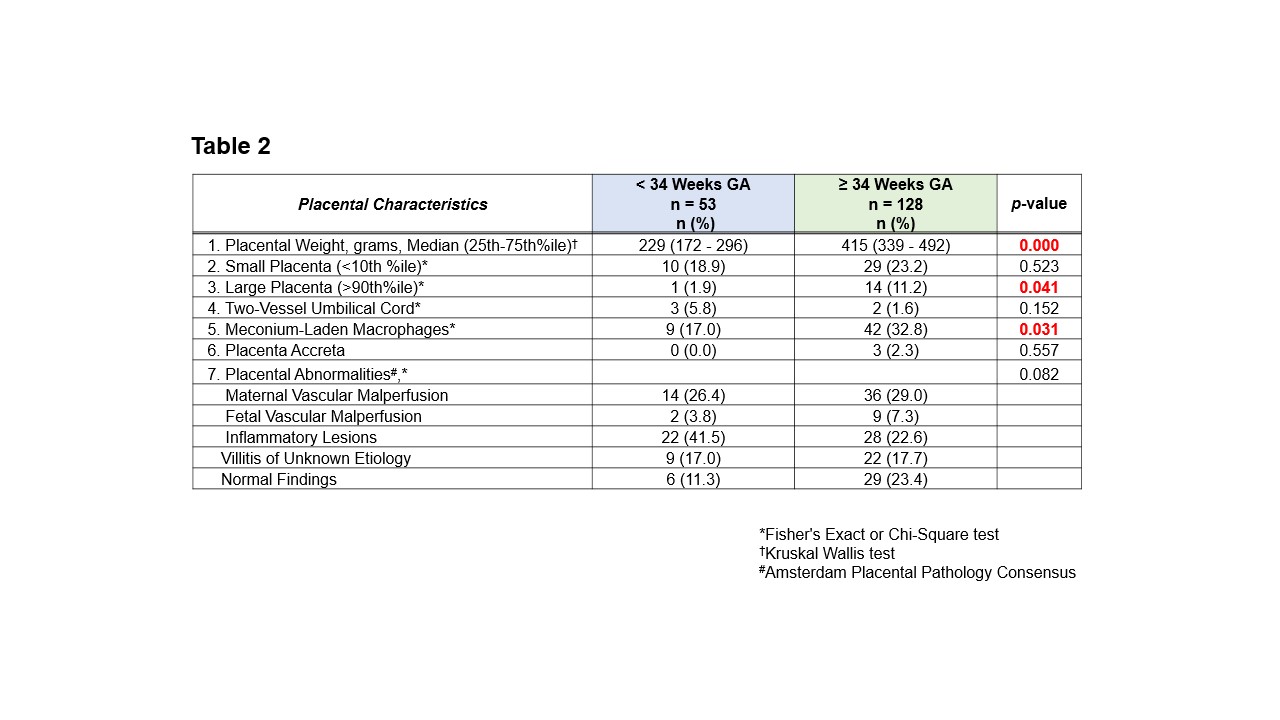 Comparison of placental pathology differences between the two groups [ < 34 weeks (PT) vs. ≥ 34 weeks (LPT/T)], with placental abnormalities categorized according to the Amsterdam Placental Pathology Consensus. Significant p-values are highlighted in bold red.
Comparison of placental pathology differences between the two groups [ < 34 weeks (PT) vs. ≥ 34 weeks (LPT/T)], with placental abnormalities categorized according to the Amsterdam Placental Pathology Consensus. Significant p-values are highlighted in bold red.