
Neonatal General 11
Session: Neonatal General 11
Katrin Lichtsinn, MD, MS (she/her/hers)
Assistant Professor of Pediatrics
Seattle Children's
Seattle, Washington, United States
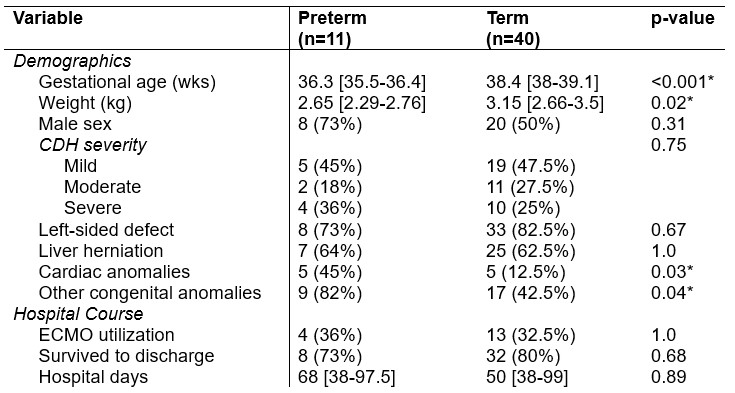 Data is represented as median [IQR] or count (%). Asterisks (*) denote results with statistical significance (p < 0.05).
Data is represented as median [IQR] or count (%). Asterisks (*) denote results with statistical significance (p < 0.05).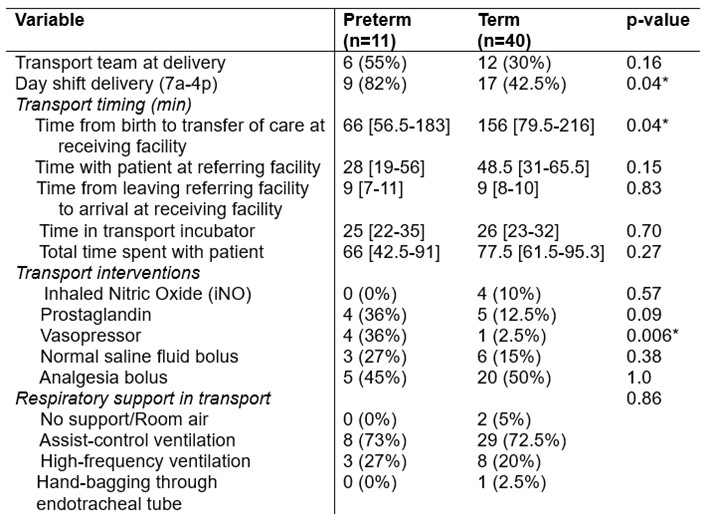 Data is represented as median [IQR] or count (%). Asterisks (*) denote results with statistical significance (p < 0.05).
Data is represented as median [IQR] or count (%). Asterisks (*) denote results with statistical significance (p < 0.05).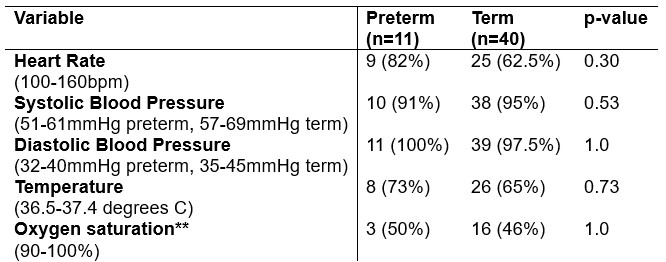 Appropriate ranges listed below each vital sign variable; any value outside of these ranges was considered abnormal. Data is represented as count (%). A single asterisk (*) denotes results with statistical significance (p < 0.05). **Oxygen saturation data removed for infants with cardiac lesions: n=5 removed preterm infants, n=5 removed term infants.Data is represented as median [IQR] or count (%). Asterisks (*) denote results with statistical significance (p < 0.05).Data is represented as median [IQR] or count (%). Asterisks (*) denote results with statistical significance (p < 0.05).Appropriate ranges listed below each vital sign variable; any value outside of these ranges was considered abnormal. Data is represented as count (%). A single asterisk (*) denotes results with statistical significance (p < 0.05). **Oxygen saturation data removed for infants with cardiac lesions: n=5 removed preterm infants, n=5 removed term infants.
Appropriate ranges listed below each vital sign variable; any value outside of these ranges was considered abnormal. Data is represented as count (%). A single asterisk (*) denotes results with statistical significance (p < 0.05). **Oxygen saturation data removed for infants with cardiac lesions: n=5 removed preterm infants, n=5 removed term infants.Data is represented as median [IQR] or count (%). Asterisks (*) denote results with statistical significance (p < 0.05).Data is represented as median [IQR] or count (%). Asterisks (*) denote results with statistical significance (p < 0.05).Appropriate ranges listed below each vital sign variable; any value outside of these ranges was considered abnormal. Data is represented as count (%). A single asterisk (*) denotes results with statistical significance (p < 0.05). **Oxygen saturation data removed for infants with cardiac lesions: n=5 removed preterm infants, n=5 removed term infants.