147 - Safety Plan Use in a Pediatric and Adolescent Primary Care Clinic
Monday, April 28, 2025
7:00am - 9:15am HST
Publication Number: 147.6313
Jasmine M. Reese, Johns Hopkins All Children's Hospital, St. Petersburg, FL, United States; Sarah Sobalvarro, Johns Hopkins All Children's Hospital, St. Petersburg, FL, United States; Alexis Dosal, Audra Walsh Psychology Group, Saint Petersburg, FL, United States; Carly M. Reeves, Tampa General Hospital Children's Medical Center, Tampa, FL, United States
Assistant Professor of Pediatrics Johns Hopkins All Children's Hospital St. Petersburg, Florida, United States
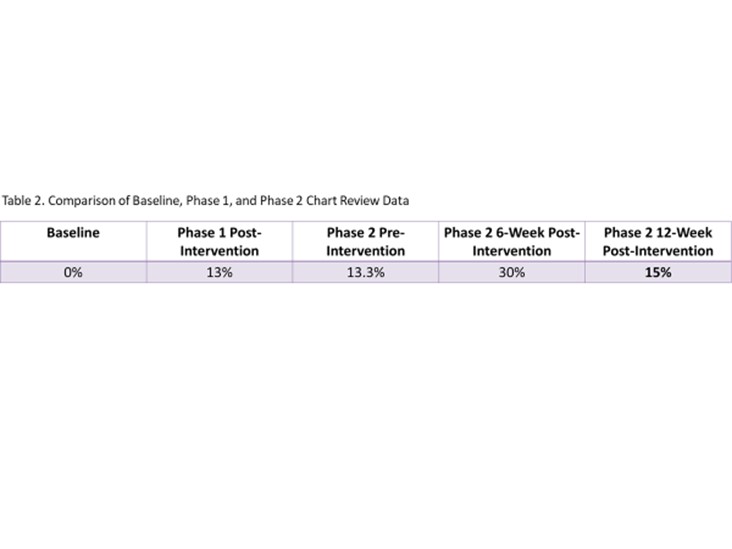
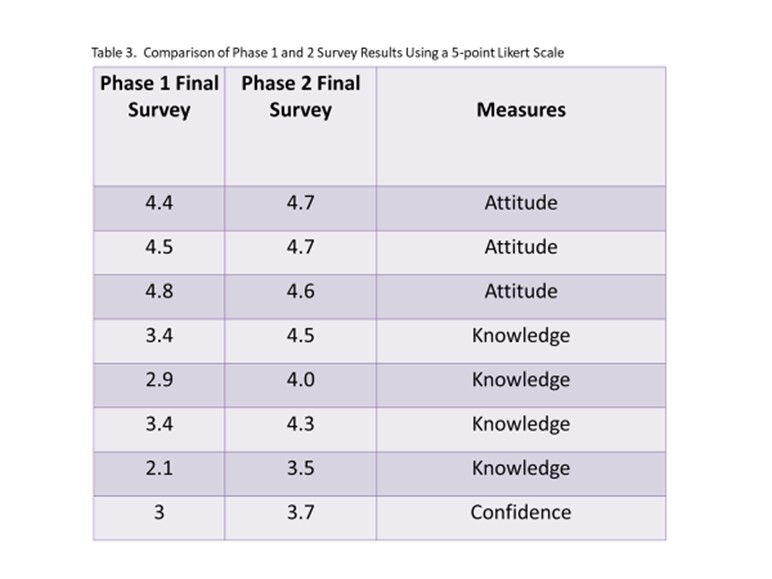
Background: Depression is a growing concern in the United States and the second leading cause of death in adolescents. Safety plans are tools supported by the American Academy of Pediatrics aimed at preventing teens from harming themselves in times of crisis. Research shows safety plans are effective at preventing suicidal behaviors but are not always utilized. Safety plans consist of six steps for individuals to take including identifying warning signs and coping strategies, identifying people and professionals to seek help from, creating a safe environment, and listing reasons for living. Objective: The aim of this project was to increase pediatric and adolescent providers’ attitudes, knowledge, comfort, and use of safety plans through educational interventions. Design/Methods: Inclusion criteria included residents, attending physicians, nurse practitioners in the pediatric primary care clinic. Screening for patient safety plan use included chart review of patients between 12 and 18 years old with at least one of 22 ICD-10 diagnosis codes related to depression during their clinic visit. Safety plan education sessions and creation of dot phrase “.SAFETYPLAN” into medical record were shared with providers. 30 randomized patient charts were assessed at 6- and 12-week intervals for documentation of safety plans. Safety plans were reviewed in 3 areas of the patient chart: flowsheet, media tab, and progress note. 5-point Likert scale surveys assessing provider attitude, knowledge and confidence were developed and distributed using Qualtrics. Results: Provider attitudes towards safety plans increased from 4.57 to 4.66, provider knowledge increased from 2.95 to 4.08, and provider confidence increased from 3 to 3.7. Baseline review showed 0% of charts documenting safety plan. After Phase 1, 13% of charts mentioned the creation of a safety plan. After Phase 2, 15% of charts mentioned safety plan use. The Phase 2 6-week chart review showed 30% safety plan use.
Conclusion(s): Provider education on safety plans is beneficial to improvement in providers’ knowledge and use of safety plans in at-risks patients. Future goals for continued progress in provision of safety plans include routine education sessions, partnering with other clinical team members (i.e. nurses, social workers) and implementation of automated reminders on the electronic medical record to document safety plans.
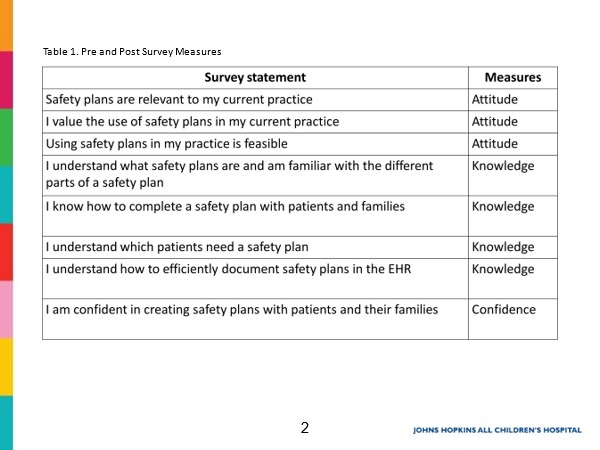
Pre and Post Survey Measures
Comparison of Baseline, Phase 1, and Phase 2 Chart Review Data
Comparison of Phase 1 and 2 Survey Results Using a 5-point Likert Scale

 photo")