
Critical Care 3
Session: Critical Care 3
 photo")
Kristin M. DeMayo, DO (she/her/hers)
Resident Physician
USF Health Morsani College of Medicine
st. petersburg, Florida, United States
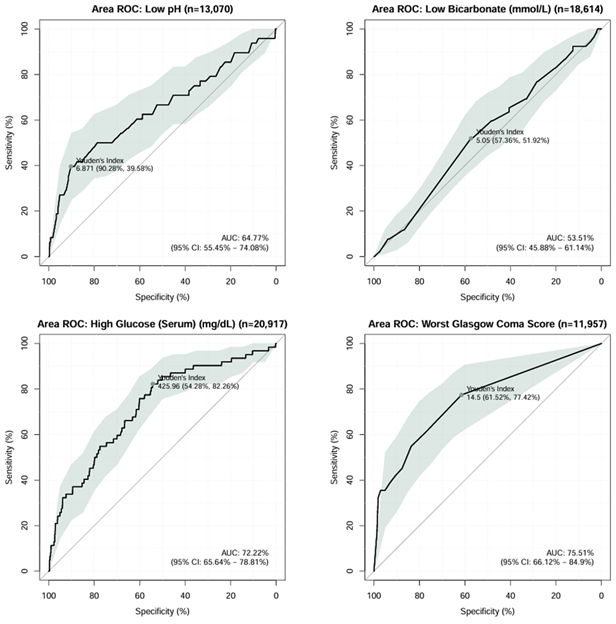 Receiver operator characteristic curve analyses for lowest pH, bicarbonate, Glasgow Coma Scale, and serum glucose within 24-hours of admission among critically ill children and young adults with diabetic ketoacidosis reporting area under the curve with 95% confidence interval, Youden’s index threshold value, and accompanying sensitivity and specific values.
Receiver operator characteristic curve analyses for lowest pH, bicarbonate, Glasgow Coma Scale, and serum glucose within 24-hours of admission among critically ill children and young adults with diabetic ketoacidosis reporting area under the curve with 95% confidence interval, Youden’s index threshold value, and accompanying sensitivity and specific values.