
Emergency Medicine 13
Session: Emergency Medicine 13
 photo")
Michael A. Gardiner, MD (he/him/his)
Associate Clinical Professor
University of California, San Diego School of Medicine
Santee, California, United States
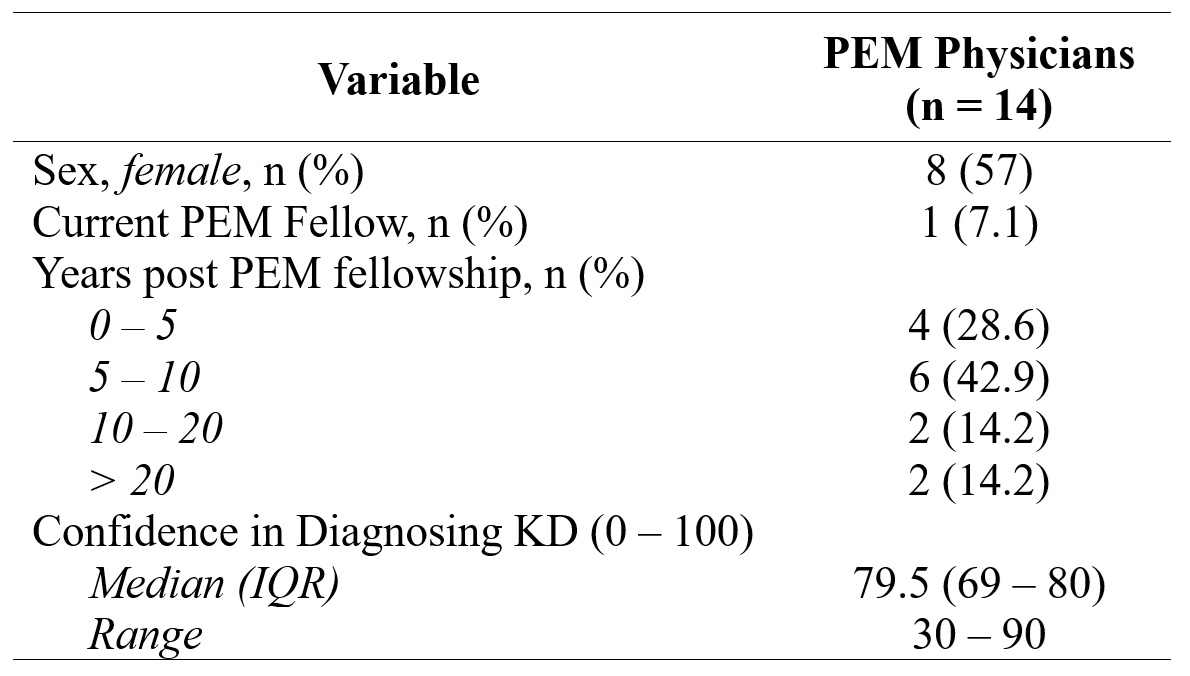 Characteristics of Physicians Completing Kawasaki Disease and Febrile Control Patient Vignettes
Characteristics of Physicians Completing Kawasaki Disease and Febrile Control Patient Vignettes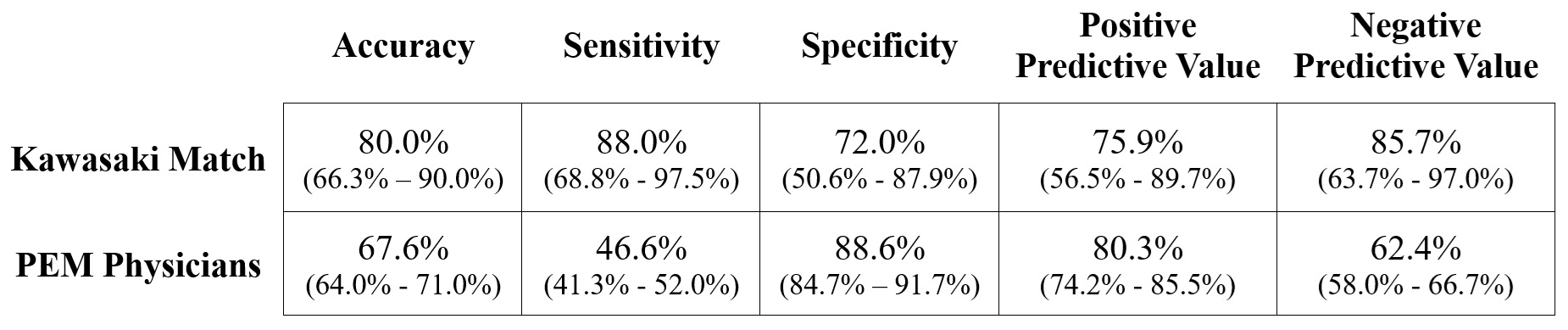 Performance Characteristics of Kawasaki Match vs. PEM Physicians (95% CI).
Performance Characteristics of Kawasaki Match vs. PEM Physicians (95% CI).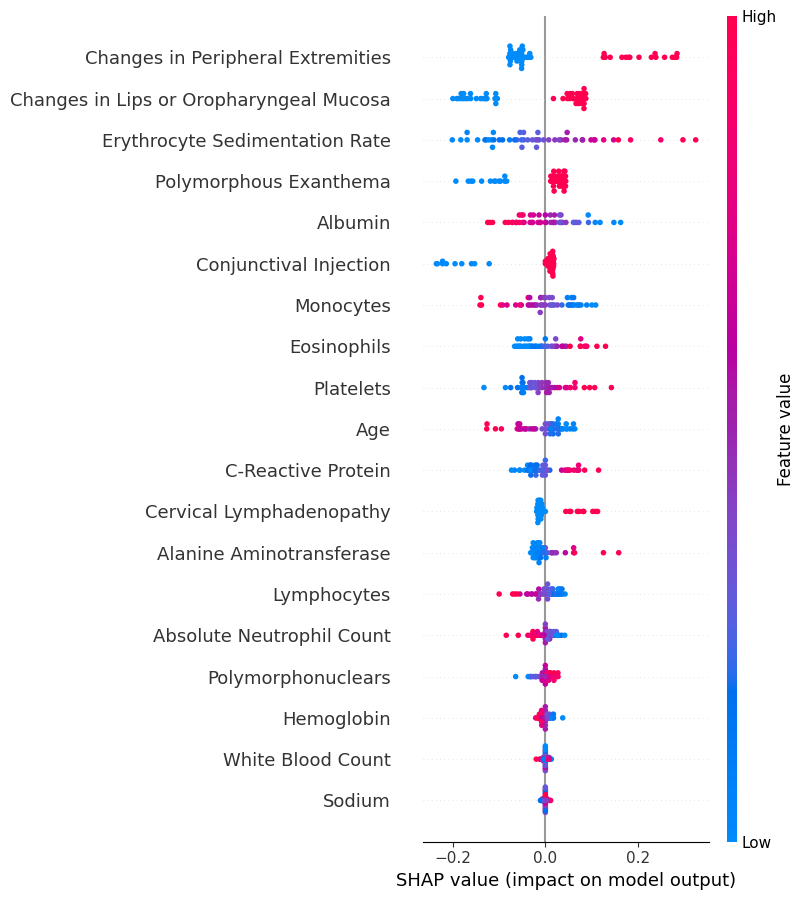 Shapley Additive Explanations (SHAP) summary plot for Kawasaki Match analysis of case vignettes. A feature for a subject with a SHAP value < 0 decreases the risk score, value > 0 increases the risk score. A higher risk score indicates a higher probability of Kawasaki Disease. Features ranked in order of importance from top to bottom.
Shapley Additive Explanations (SHAP) summary plot for Kawasaki Match analysis of case vignettes. A feature for a subject with a SHAP value < 0 decreases the risk score, value > 0 increases the risk score. A higher risk score indicates a higher probability of Kawasaki Disease. Features ranked in order of importance from top to bottom.