
Adolescent Medicine 5: Potpourri
Session: Adolescent Medicine 5: Potpourri
 photo")
Jessica Kahn, MD MPH (she/her/hers)
Senior Associate Dean for Clinical and Translational Research
Albert Einstein College of Medicine
Bronx, New York, United States
.png) Prevalence of HPV35, 39, 59, 67, 68, and/or 70 (alpha 9 and 7 types genetically related to HPV16 and HPV18 but not targeted by the 4-valent or 9-valent HPV vaccine) by vaccination status, propensity score adjusted: to assess for cross-protection
Prevalence of HPV35, 39, 59, 67, 68, and/or 70 (alpha 9 and 7 types genetically related to HPV16 and HPV18 but not targeted by the 4-valent or 9-valent HPV vaccine) by vaccination status, propensity score adjusted: to assess for cross-protection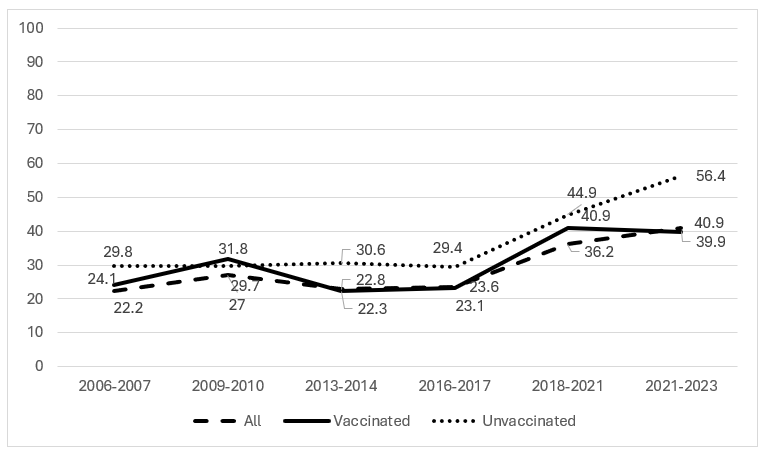 Prevalence of HPV26, 51, 53, 56, 66, 69, 82, and/or 73 (alpha 5, 6, and 11 types not genetically related to types targeted by the 4-valent or 9-valent HPV vaccine) by vaccination status, propensity score adjusted: to assess for type replacement
Prevalence of HPV26, 51, 53, 56, 66, 69, 82, and/or 73 (alpha 5, 6, and 11 types not genetically related to types targeted by the 4-valent or 9-valent HPV vaccine) by vaccination status, propensity score adjusted: to assess for type replacement Test of linear trend across surveillance studies, propensity score adjusted, using surveillance study as a continuous variable: outcomes are prevalence of alpha 9 and 7 types genetically related to HPV16 and HPV18 but not targeted by the 4-valent or 9-valent HPV vaccine (to assess for cross-protection), and prevalence of alpha 5, 6, and 11 types not genetically related to types targeted by the 4-valent or 9-valent HPV vaccine (to assess for type replacement)Prevalence of HPV35, 39, 59, 67, 68, and/or 70 (alpha 9 and 7 types genetically related to HPV16 and HPV18 but not targeted by the 4-valent or 9-valent HPV vaccine) by vaccination status, propensity score adjusted: to assess for cross-protectionPrevalence of HPV26, 51, 53, 56, 66, 69, 82, and/or 73 (alpha 5, 6, and 11 types not genetically related to types targeted by the 4-valent or 9-valent HPV vaccine) by vaccination status, propensity score adjusted: to assess for type replacementTest of linear trend across surveillance studies, propensity score adjusted, using surveillance study as a continuous variable: outcomes are prevalence of alpha 9 and 7 types genetically related to HPV16 and HPV18 but not targeted by the 4-valent or 9-valent HPV vaccine (to assess for cross-protection), and prevalence of alpha 5, 6, and 11 types not genetically related to types targeted by the 4-valent or 9-valent HPV vaccine (to assess for type replacement)
Test of linear trend across surveillance studies, propensity score adjusted, using surveillance study as a continuous variable: outcomes are prevalence of alpha 9 and 7 types genetically related to HPV16 and HPV18 but not targeted by the 4-valent or 9-valent HPV vaccine (to assess for cross-protection), and prevalence of alpha 5, 6, and 11 types not genetically related to types targeted by the 4-valent or 9-valent HPV vaccine (to assess for type replacement)Prevalence of HPV35, 39, 59, 67, 68, and/or 70 (alpha 9 and 7 types genetically related to HPV16 and HPV18 but not targeted by the 4-valent or 9-valent HPV vaccine) by vaccination status, propensity score adjusted: to assess for cross-protectionPrevalence of HPV26, 51, 53, 56, 66, 69, 82, and/or 73 (alpha 5, 6, and 11 types not genetically related to types targeted by the 4-valent or 9-valent HPV vaccine) by vaccination status, propensity score adjusted: to assess for type replacementTest of linear trend across surveillance studies, propensity score adjusted, using surveillance study as a continuous variable: outcomes are prevalence of alpha 9 and 7 types genetically related to HPV16 and HPV18 but not targeted by the 4-valent or 9-valent HPV vaccine (to assess for cross-protection), and prevalence of alpha 5, 6, and 11 types not genetically related to types targeted by the 4-valent or 9-valent HPV vaccine (to assess for type replacement)