475 - Frequency of Technology Dependence in Hospitalized Children by Hospital Type and Teaching Status
Monday, April 28, 2025
7:00am - 9:15am HST
Publication Number: 475.4641
Emily J. Goodwin, CMKC, Kansas City, MO, United States; Isabella Zaniletti, IZ Statistics LLC, Tampa, FL, United States; S. Margaret Wright, Children's Mercy Kansas City, Kansas City, MO, United States; Jeffrey Colvin, Children's Mercy Hospitals and Clinics, Kansas City, MO, United States; Matthew Hall, Children's Hospital Association, Lenexa, KS, United States
Associate Professor or Pediatrics Children's Mercy Kansas City Kansas City, Missouri, United States
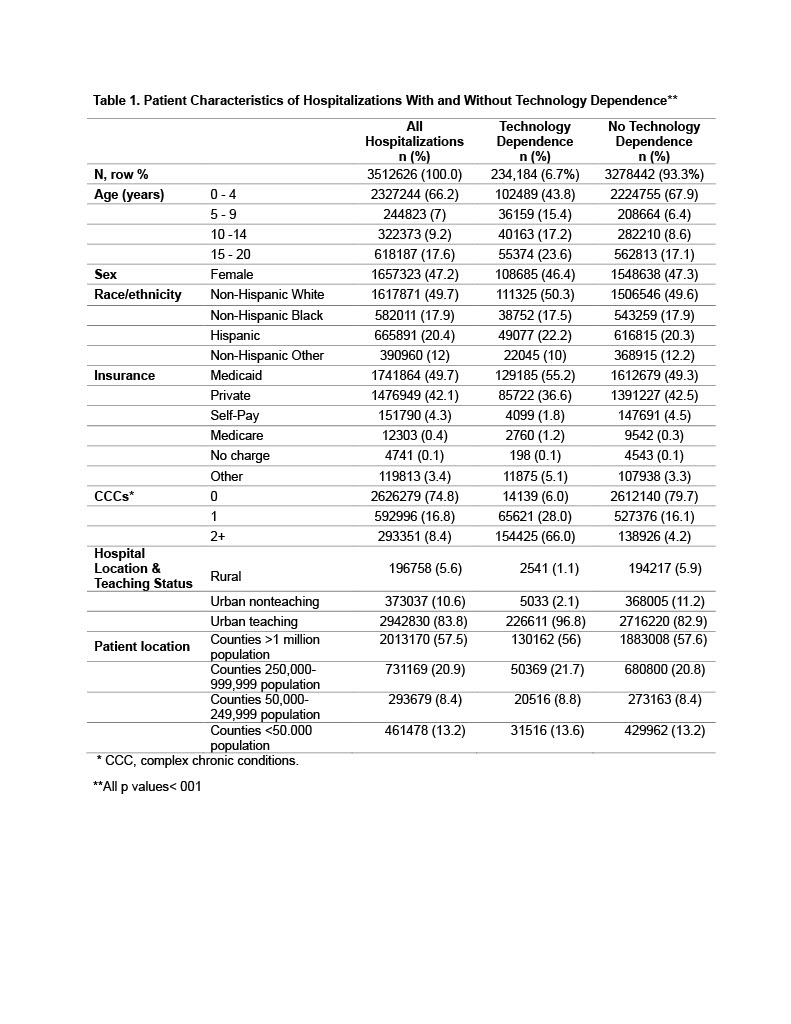
Background: Hospitals and medical professionals need to be prepared to care for children with technology dependence (TD). However, where children with TD seek care when they require hospitalization is unknown, including if they are admitted to rural compared to urban hospitals. Objective: To determine 1) the frequency of pediatric inpatient discharges with TD by rural/urban location and teaching status of hospital and 2) the most frequent types of TD within each type of hospital. Design/Methods: We performed a retrospective cross-sectional study of the 2019 Kids’ Inpatient Database (KID), the largest pediatric all-payer inpatient sample database. The KID includes all acute care hospital types and is weighted to make national estimates. We excluded admissions for uncomplicated newborns and obstetrics/gynecology-related conditions. Feudtner’s Complex Chronic Condition (CCC) classification system version 3 was used to identify children with TD. We categorized TD into 54 distinct TD types. We used weights to determine frequencies and percentages of pediatric inpatient discharges with TD by location/teaching status of hospital (rural, urban nonteaching, urban teaching) and chi square tests to test differences between groups. Results: Of the 3.5 million weighted discharges included, 6.7% (95% CI: 6.1%-7.2%) had ≥1 TD (Table 1). A higher percentage of discharges with TD had ≥1 CCC (94.0% vs. 20.3%, p<.001) and relied on Medicaid (55.2% vs. 49.2%, p< 0.001). The most common types of TD were gastrostomy tubes (3.2% of all discharges) followed by ventricular shunts (0.9%), and tracheostomies (0.8%) (Table 2). While gastrostomy tubes were the most common TD at all hospital types, rural hospitals had a lower frequency of hospitalizations with tracheostomy tubes, ventilators, vascular access devices, and other cardiac technology compared to urban hospitals. Approximately 13% of hospitalizations with TD were children that live in rural areas ( < 50,000 population). Among discharges with TD, 1.1% were from rural hospitals, 2.1% from urban nonteaching, and 96.8% from urban teaching hospitals.
Conclusion(s): Approximately 1 in 20 pediatric inpatient discharges had TD, with gastrostomy tubes being the most common TD type. Among discharges with TD, most presented to urban teaching hospitals with approximately 13% of those children residing in rural areas. Understanding the most common types of TD is important for improving preparedness of clinical teams including resource allocation and training in caring for children with TD.
TABLE 1: Patient Characteristics of Hospitalizations With and Without Technology Dependence
Table 2 The Most Frequent Technology Dependency Types Among Pediatric Hospitalizations by Hospital Location and Teaching Status
TABLE 1: Patient Characteristics of Hospitalizations With and Without Technology Dependence
Table 2 The Most Frequent Technology Dependency Types Among Pediatric Hospitalizations by Hospital Location and Teaching Status

 photo")
.jpg)
