
Critical Care 4
Session: Critical Care 4
 photo")
Austin McCuistion, MD (he/him/his)
Pediatric Nephrology Fellow
Children's Hospital Colorado
Denver, Colorado, United States
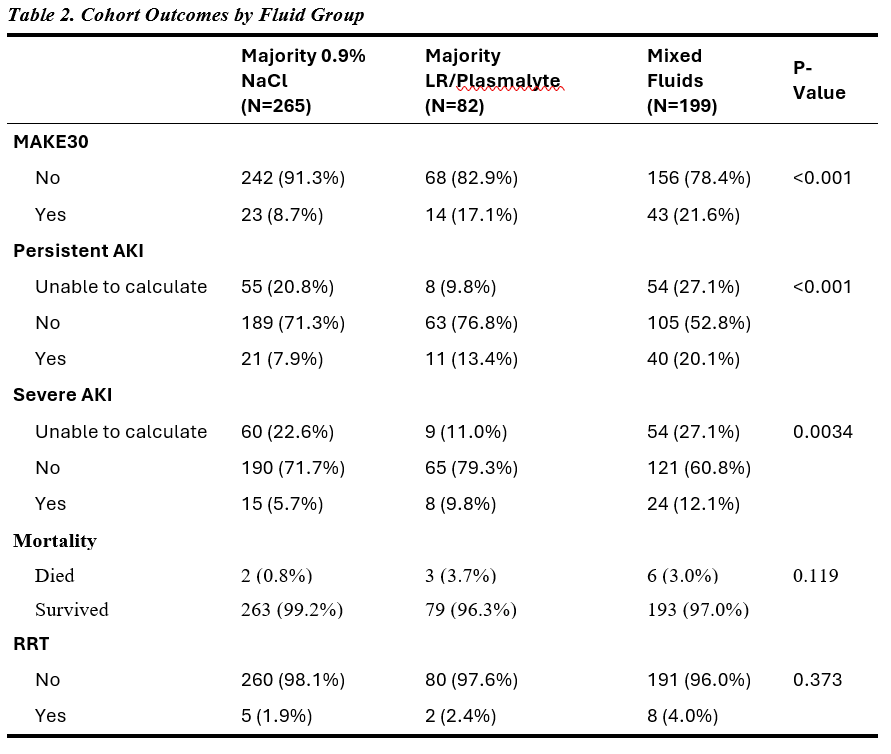
 Logistic regression comparing MAKE30 between LR and Mixed fluid with NS group after controlling for age, sex, site, and PRISM score.
Logistic regression comparing MAKE30 between LR and Mixed fluid with NS group after controlling for age, sex, site, and PRISM score.