
Critical Care 4
Session: Critical Care 4
 photo")
Rezvaneh Ghasemzadeh, MD (she/her/hers)
Pediatric Critical Care Fellow
University of California, San Francisco, School of Medicine
Oakland, California, United States
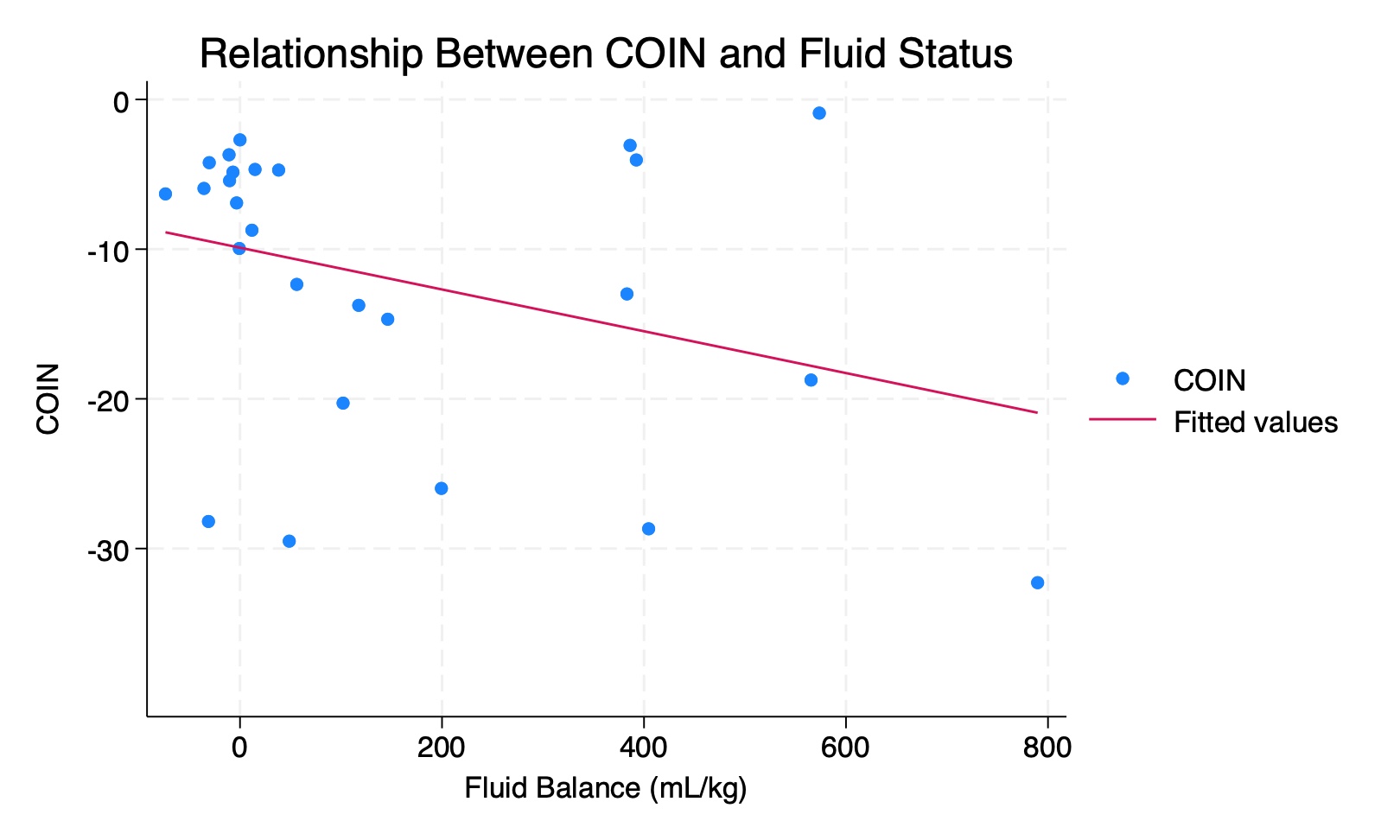 Relationship between COIN and fluid balance at the time of ECLS cannulation.
Relationship between COIN and fluid balance at the time of ECLS cannulation.