
Neonatal Pulmonology - Basic/Translational Science 3
Session: Neonatal Pulmonology - Basic/Translational Science 3
 photo")
Susan S. Kim, MD (she/her/hers)
Neonatal Fellow
Icahn School of Medicine at Mount Sinai
New York, New York, United States
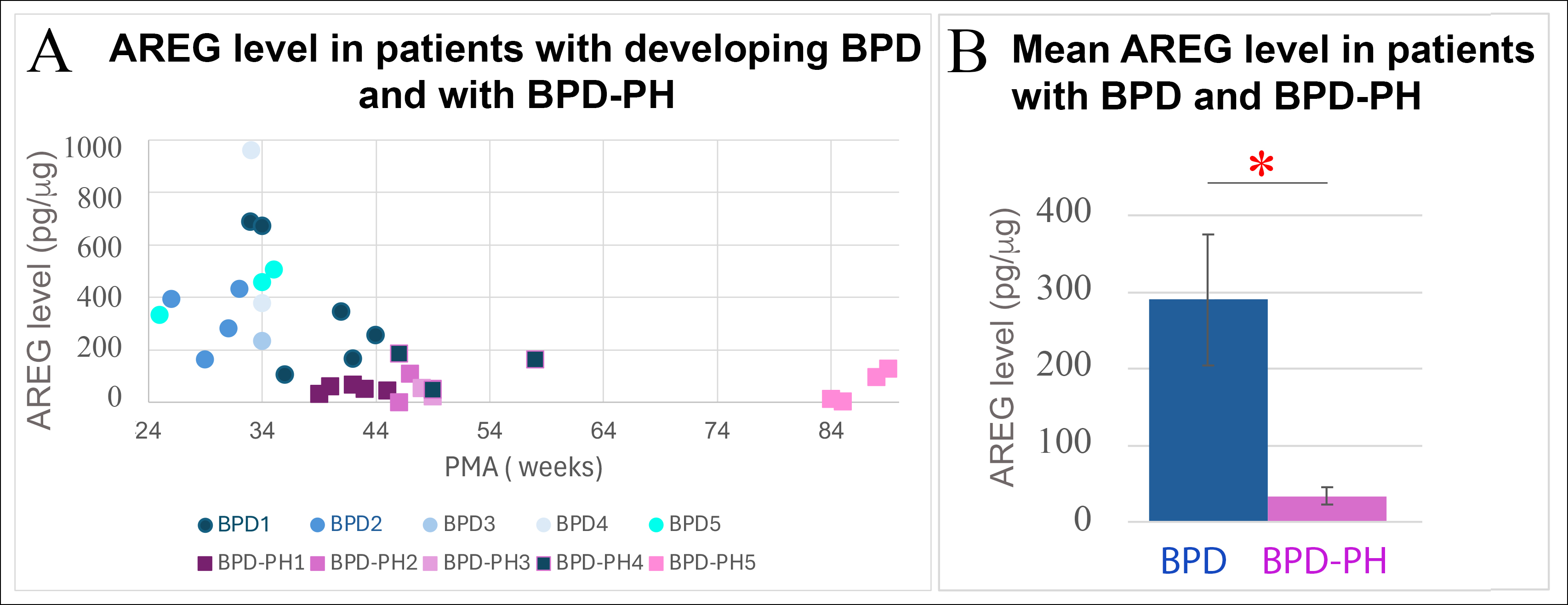 Panel A) AREG levels in TAs of 9 infants with developing BPD and BPD-PH at different PMAs. One infant (BPD1) developed PH (BPD-PH4). Panel B) AREG level in patients affected by BPD (n=4) and BPD-PH (n=4) born at the same GA and measured at the same PMA. * p<0.05. PMA = postmenstrual age.
Panel A) AREG levels in TAs of 9 infants with developing BPD and BPD-PH at different PMAs. One infant (BPD1) developed PH (BPD-PH4). Panel B) AREG level in patients affected by BPD (n=4) and BPD-PH (n=4) born at the same GA and measured at the same PMA. * p<0.05. PMA = postmenstrual age. 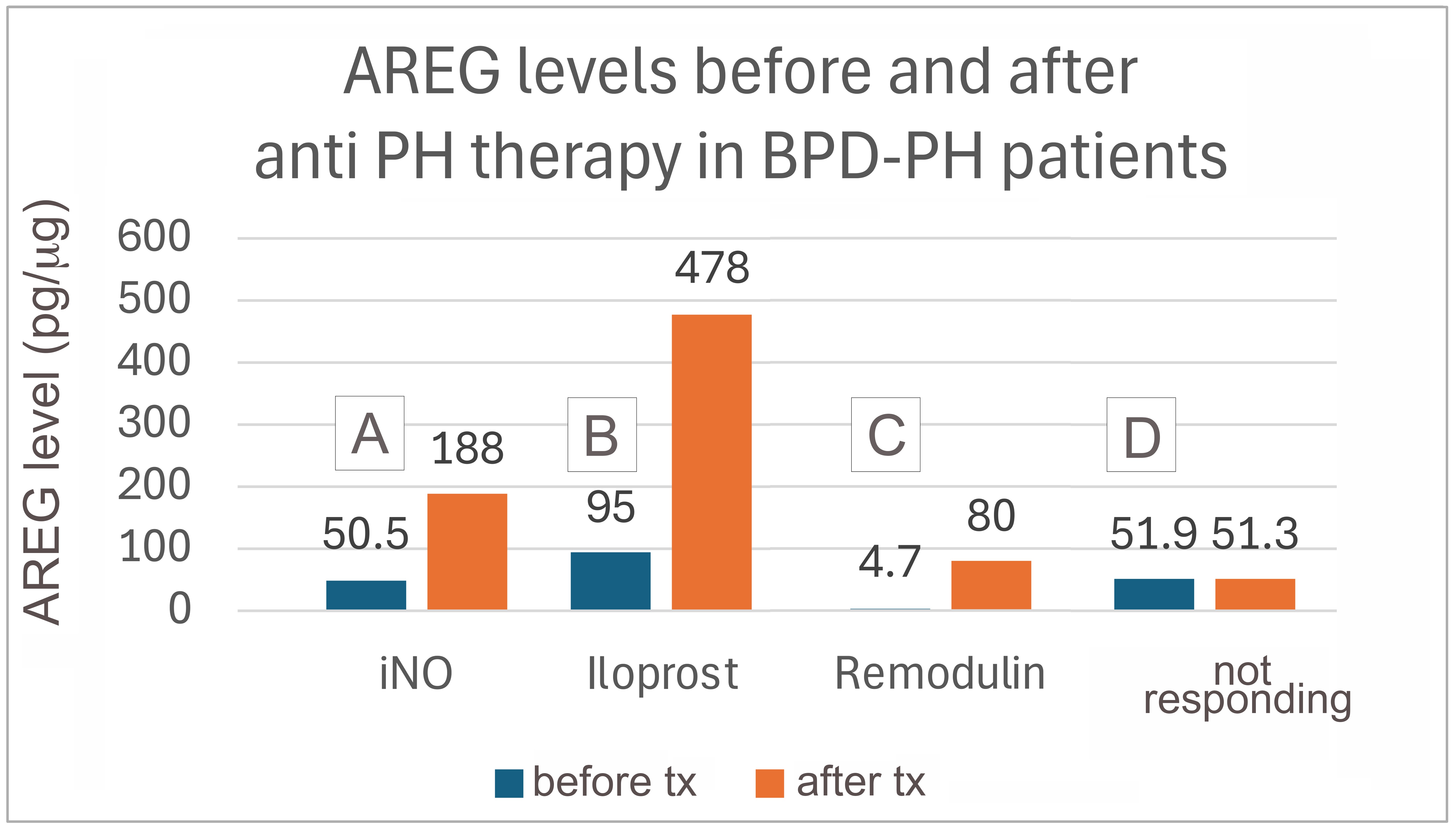 AREG levels before and after different PH therapies in infants with BPD-PH.
AREG levels before and after different PH therapies in infants with BPD-PH. 