
Emergency Medicine 14
Session: Emergency Medicine 14
 photo")
Vitaliy Perepelitsa, DO (he/him/his)
Resident physician
University of Minnesota Masonic Children's Hospital
Minneapolis, Minnesota, United States
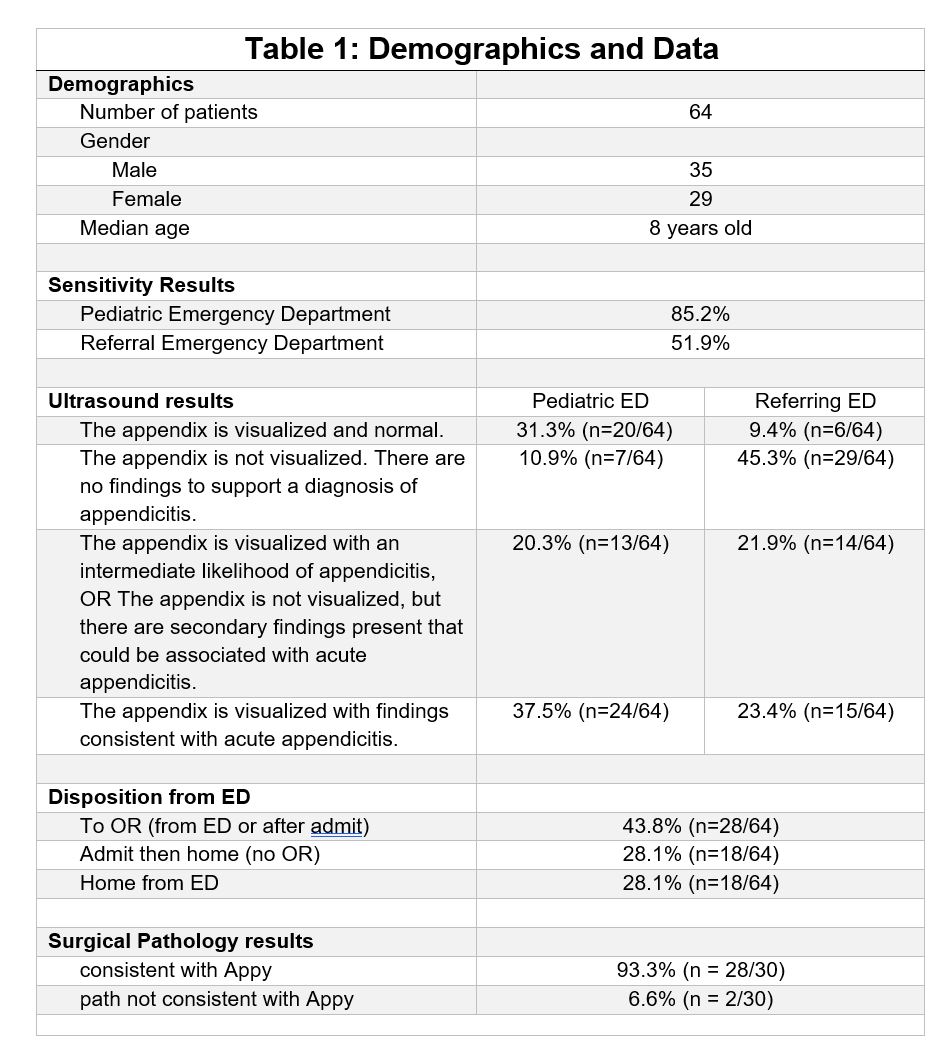 Demographics and DataDemographics and Data
Demographics and DataDemographics and Data