
Health Equity/Social Determinants of Health 10
Session: Health Equity/Social Determinants of Health 10
 Credit")
 photo")
Kaitlyn Sacotte, MD (she/her/hers)
Neonatal-Perinatal Medicine Fellow
University of Utah
Salt Lake City, Utah, United States
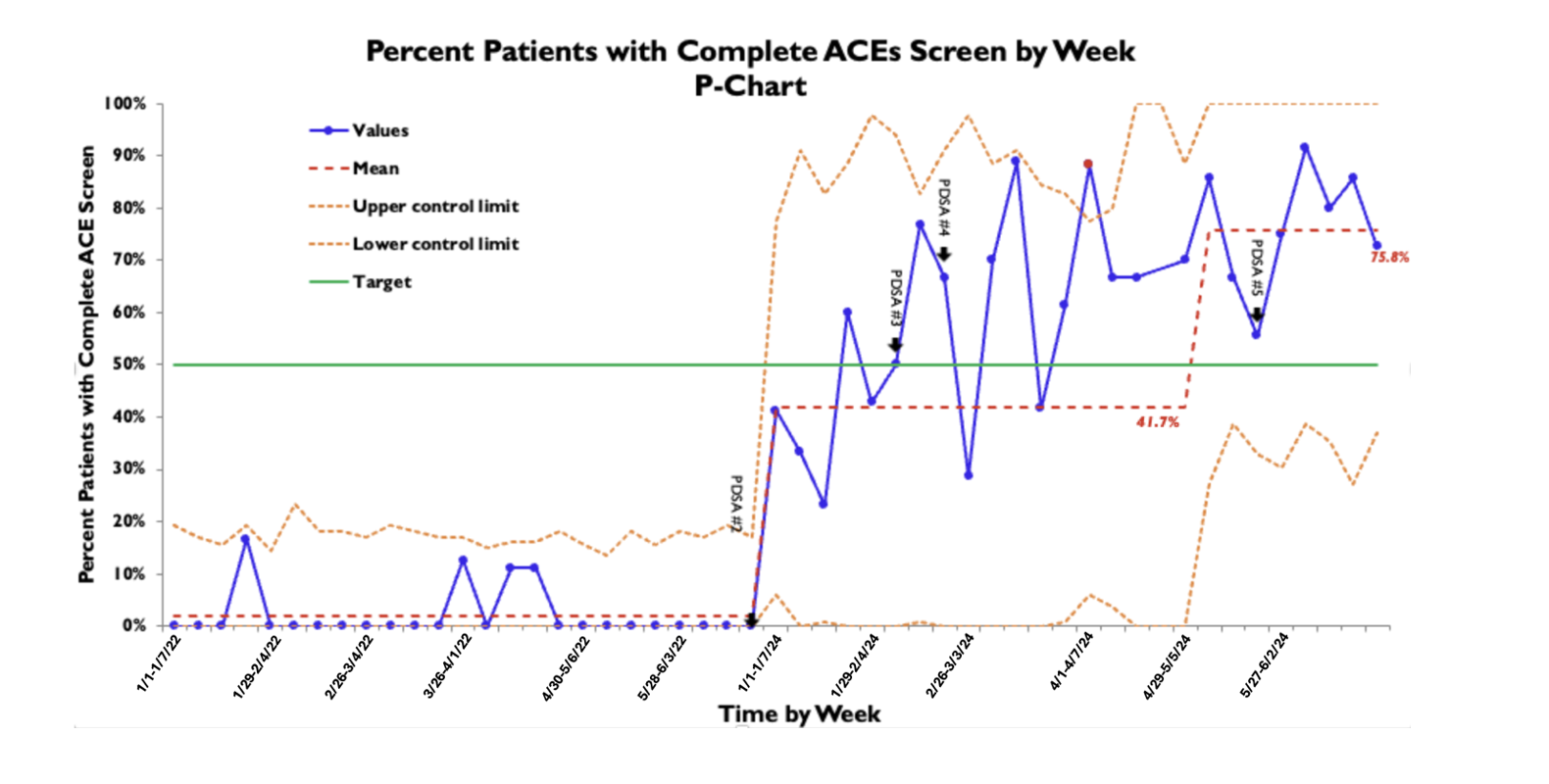 Each data point represents a week, with the first week of the month denoted with the date.Each data point represents a week, with the first week of the month denoted with the date.
Each data point represents a week, with the first week of the month denoted with the date.Each data point represents a week, with the first week of the month denoted with the date.