
Mental Health 3
Session: Mental Health 3
.jpg "Stephanie C. Acquilano, MA (she/her/hers) photo")
Stephanie C. Acquilano, MA (she/her/hers)
Research Project Director
Geisel School of Medicine at Dartmouth
Lebanon, New Hampshire, United States
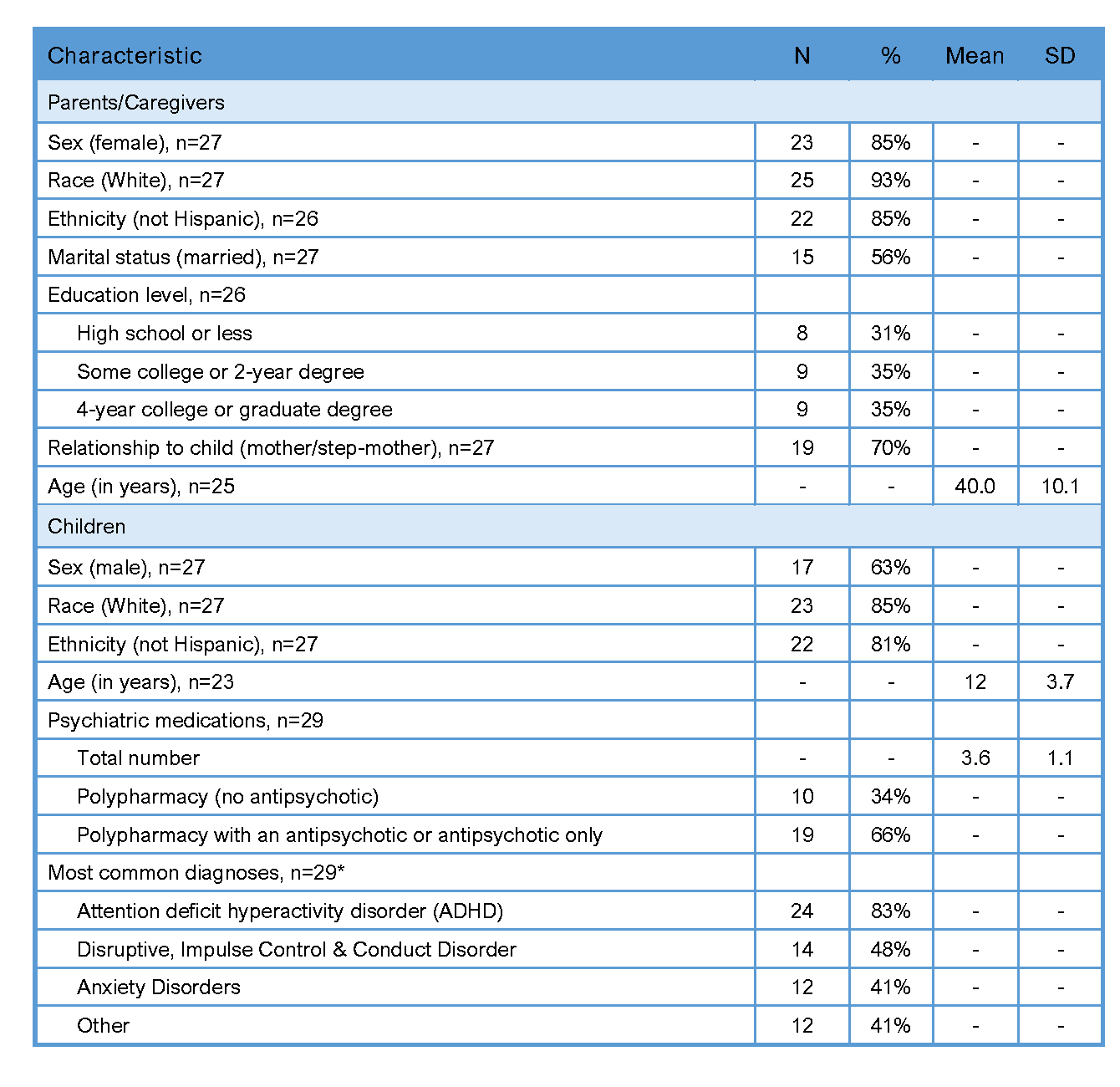 Note: SD = standard deviation, polypharmacy = 3 or more medications.
Note: SD = standard deviation, polypharmacy = 3 or more medications.