
Critical Care 4
Session: Critical Care 4
 photo")
Alyssa Mueller, MD (she/her/hers)
Resident
Monroe Carell Jr. Children's Hospital at Vanderbilt
Nashville, Tennessee, United States
.png) ECMO = extracorporeal membrane oxygenation, PT = physical therapy, OT = occupational therapy, FSS = fatigue severity scale, PAMS = physical abilities and mobility scale
ECMO = extracorporeal membrane oxygenation, PT = physical therapy, OT = occupational therapy, FSS = fatigue severity scale, PAMS = physical abilities and mobility scale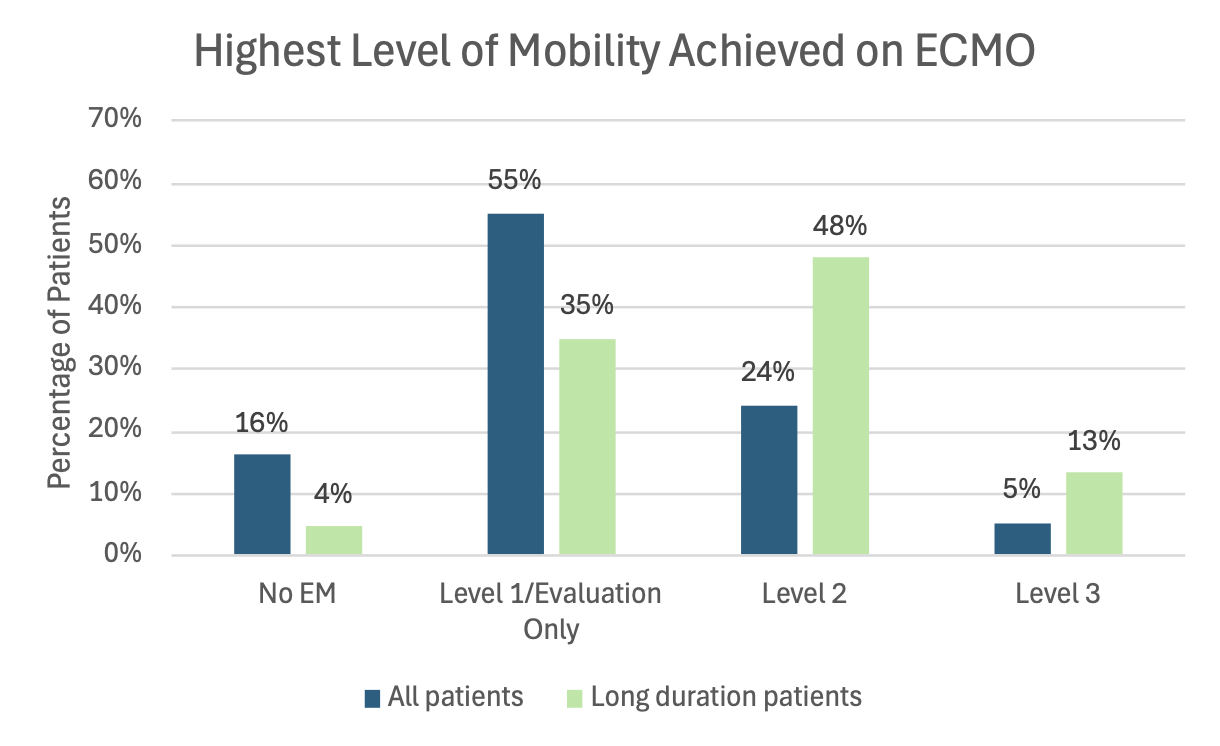 Levels based on institutional protocol. ECMO = extracorporeal membrane oxygenation, PT = physical therapy, OT = occupational therapy, FSS = fatigue severity scale, PAMS = physical abilities and mobility scaleLevels based on institutional protocol.
Levels based on institutional protocol. ECMO = extracorporeal membrane oxygenation, PT = physical therapy, OT = occupational therapy, FSS = fatigue severity scale, PAMS = physical abilities and mobility scaleLevels based on institutional protocol. 