
Critical Care 2
Session: Critical Care 2
 photo")
Cydni Williams, MD, MCR (she/her/hers)
Associate Professor of Pediatrics
Doernbecher Children's Hospital at Oregon Health & Science University
Portland, Oregon, United States

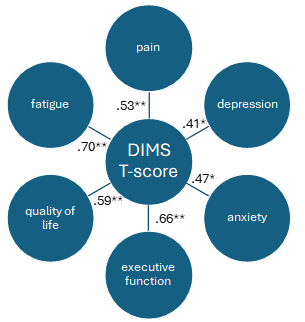 Spearman Correlations (r) between Sleep Disturbances Scale for Children Disorders of Initiation and Maintenance of Sleep (DIMS) scale and health outcomes 6-months after traumatic brain injury. *p <.05, **p <.01
Spearman Correlations (r) between Sleep Disturbances Scale for Children Disorders of Initiation and Maintenance of Sleep (DIMS) scale and health outcomes 6-months after traumatic brain injury. *p <.05, **p <.01