
Cardiology 2
Session: Cardiology 2
 photo")
Alejandra Mallorga Hernandez, MD, MPH (she/her/hers)
Resident physician
Children's Hospital Los Angeles
Los Angeles, California, United States
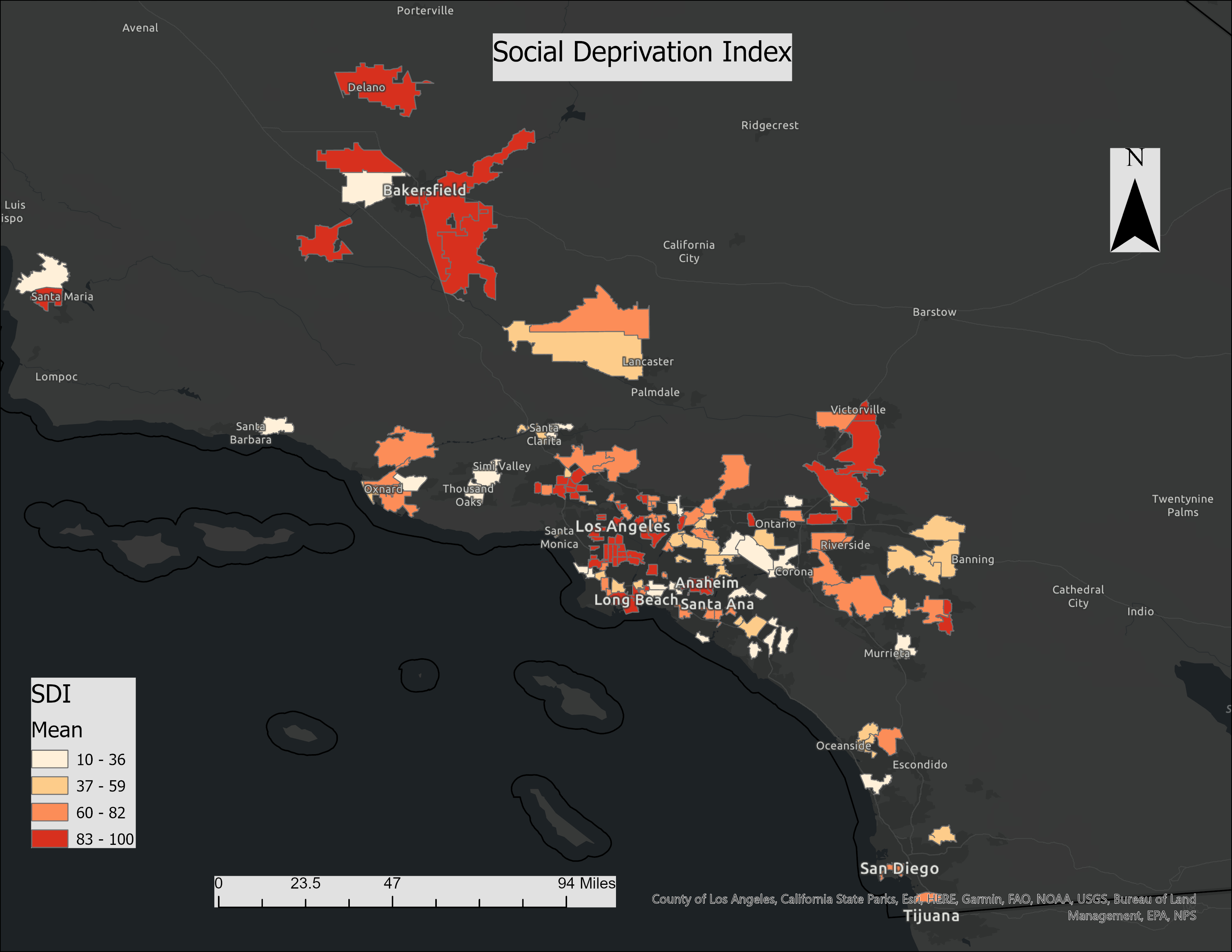 SDI is the composite measure of area level deprivation based on census data used to quantify the socio-economic variation in health outcomes. As the SDI score increases (darker shades), the severity of deprivation increases. In this figure, ArcGIS was used to map SDI for the patient population included in our study.
SDI is the composite measure of area level deprivation based on census data used to quantify the socio-economic variation in health outcomes. As the SDI score increases (darker shades), the severity of deprivation increases. In this figure, ArcGIS was used to map SDI for the patient population included in our study. .png) On the univariate analysis, CCHD category, maternal age, and insurance type were noted to have a significant effect on prenatal diagnosis of CCHD during the COVID pandemic. SDI impact on PD for all lesions as a singular group, was noted to be non-significant. However, on further multivariate analysis, it was found that while SDI did not play a key role for PD of single ventricle and OFT lesions, it significantly impacted PD for Group 3, lesions with historically lower detection rates in utero. In this group, infants with higher SES were 7 times more likely to be diagnosed prenatally (odds ratio 7.04, 95% CI, 1.6 to 31.2, p=0.0106).
On the univariate analysis, CCHD category, maternal age, and insurance type were noted to have a significant effect on prenatal diagnosis of CCHD during the COVID pandemic. SDI impact on PD for all lesions as a singular group, was noted to be non-significant. However, on further multivariate analysis, it was found that while SDI did not play a key role for PD of single ventricle and OFT lesions, it significantly impacted PD for Group 3, lesions with historically lower detection rates in utero. In this group, infants with higher SES were 7 times more likely to be diagnosed prenatally (odds ratio 7.04, 95% CI, 1.6 to 31.2, p=0.0106).