
Emergency Medicine 3
Session: Emergency Medicine 3
 photo")
Jacob Phouthavong-Murphy, DO (he/him/his)
Pediatric Resident
Phoenix Children's Hospital
Tempe, Arizona, United States
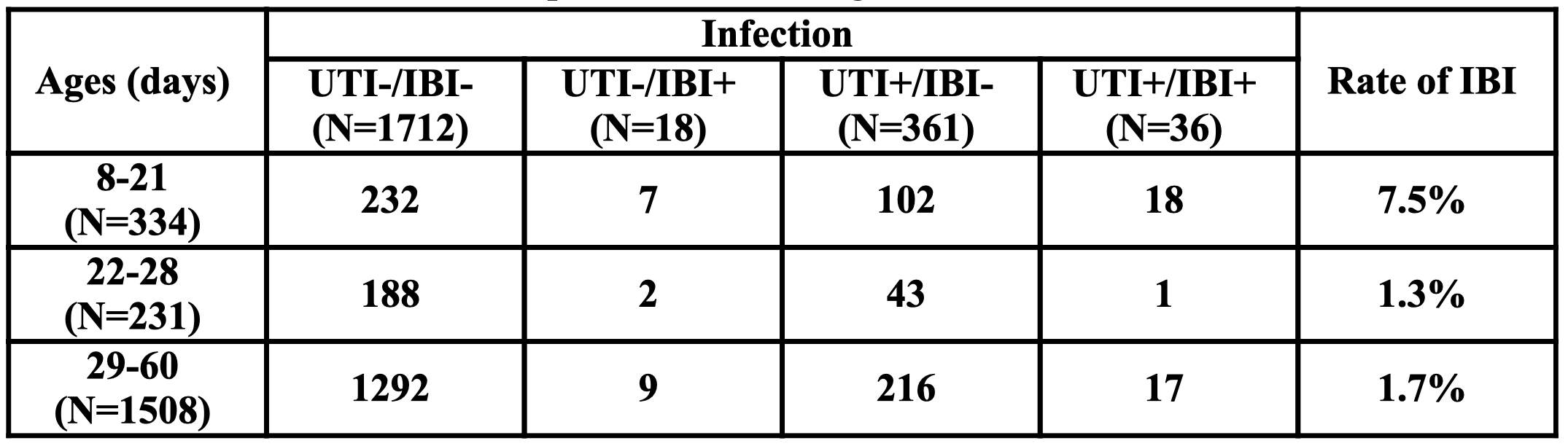 UTI: Urinary tract infection; IBI: Invasive bacterial infection (bacteremia, meningitis); N: Number of patients
UTI: Urinary tract infection; IBI: Invasive bacterial infection (bacteremia, meningitis); N: Number of patients  UTI: Urinary tract infection; IBI: Invasive bacterial infection (bacteremia, meningitis); RR: Relative risk; CI: Confidence interval
UTI: Urinary tract infection; IBI: Invasive bacterial infection (bacteremia, meningitis); RR: Relative risk; CI: Confidence interval  UTI: Urinary tract infection; IBI: Invasive bacterial infection (bacteremia, meningitis); RR: Relative risk; CI: Confidence interval
UTI: Urinary tract infection; IBI: Invasive bacterial infection (bacteremia, meningitis); RR: Relative risk; CI: Confidence interval