
Neo-Perinatal Health Care Delivery: Practices and Procedures 2
Session: Neo-Perinatal Health Care Delivery: Practices and Procedures 2
.jpg "Prakesh S. Shah, MD FRCPC (he/him/his) photo")
Prakesh S. Shah, MD FRCPC (he/him/his)
Professor
Mount Sinai Hospital
Toronto, Ontario, Canada
.png) Abbreviations: CNFUN, Canadian Neonatal Follow-Up Network
Abbreviations: CNFUN, Canadian Neonatal Follow-Up Network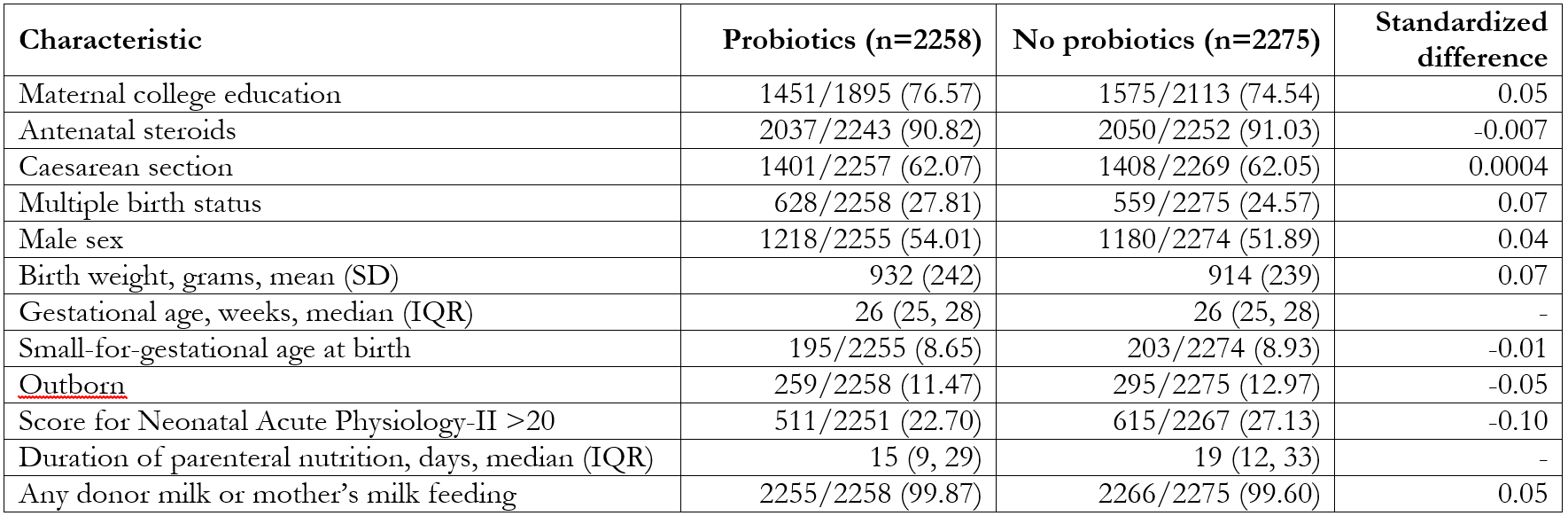 Data presented as No./Total No. (%) unless otherwise specified. Values outside of |0.1| are considered statistically significant.
Data presented as No./Total No. (%) unless otherwise specified. Values outside of |0.1| are considered statistically significant..png) Vertical dotted line in both panels represents equivalence margin of 4%.
Vertical dotted line in both panels represents equivalence margin of 4%.