
Neonatal Quality Improvement 2
Session: Neonatal Quality Improvement 2
 Credit")
Lakshmi Srinivasan, MBBS MSTR (she/her/hers)
Assistant Professor
The Children's Hospital of Philadelphia
Philadelphia, Pennsylvania, United States
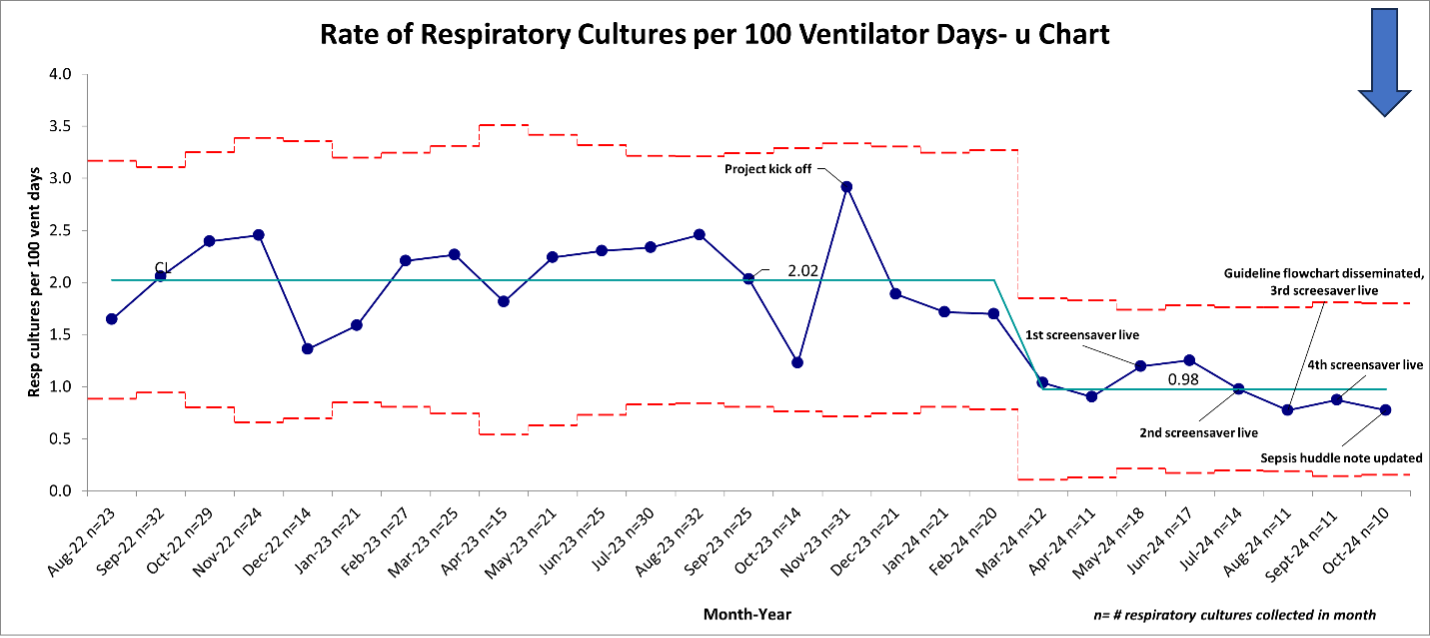 Centerline shift determined to start in March 2024, based on meeting special cause rules and QI team hypothesis about interventions contributing to shift.
Centerline shift determined to start in March 2024, based on meeting special cause rules and QI team hypothesis about interventions contributing to shift.