
Neonatal Quality Improvement 1
Session: Neonatal Quality Improvement 1
 Credit")
Emma Prichard, DO (she/her/hers)
Neonatal-Perinatal Fellow
Brooke Army Medical Center
San Antonio, Texas, United States
.png) Run chart depicting the change in percent of infants reaching STSC within 12 hours of life (blue) and number of infants without any skin to skin documented (orange) over time. A) PDSA1 - Educational materials given to nursing and NICU providers B) PDSA 2 - Intervention bundle and new protocol implemented 1JAN C) PDSA3 - Charge nurse champions D) PDSA 4 - Monthly email updates E) PDSA 5 - Nurse shout outs implemented.
Run chart depicting the change in percent of infants reaching STSC within 12 hours of life (blue) and number of infants without any skin to skin documented (orange) over time. A) PDSA1 - Educational materials given to nursing and NICU providers B) PDSA 2 - Intervention bundle and new protocol implemented 1JAN C) PDSA3 - Charge nurse champions D) PDSA 4 - Monthly email updates E) PDSA 5 - Nurse shout outs implemented.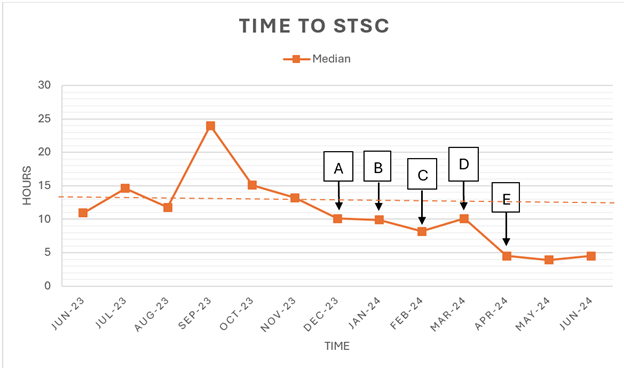 Run chart depicting the change in median time to STSC over time. A-E described in Figure 1.
Run chart depicting the change in median time to STSC over time. A-E described in Figure 1.