
Global Neonatal & Children's Health 2
Session: Global Neonatal & Children's Health 2
 photo")
Alastair Fung, MD, MPH (he/him/his)
Clinical Fellow
The Hospital for Sick Children
Toronto, Ontario, Canada
.png) a At least one sign of possible serious bacterial infection (poor feeding, convulsions, severe chest indrawing, fever (>=38oC), hypothermia ( <35.5oC), lethargy, or fast breathing (>=60 breaths per minute in infants <7 days old)) documented by a study medical officer and non-study treating physician decision to admit to hospital.
a At least one sign of possible serious bacterial infection (poor feeding, convulsions, severe chest indrawing, fever (>=38oC), hypothermia ( <35.5oC), lethargy, or fast breathing (>=60 breaths per minute in infants <7 days old)) documented by a study medical officer and non-study treating physician decision to admit to hospital.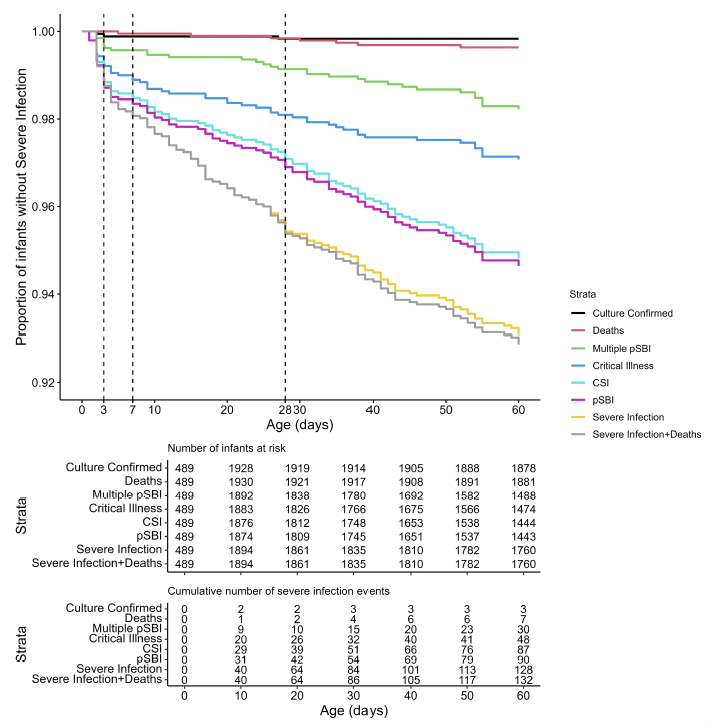 CSI: clinical severe infection; pSBI: possible serious bacterial infection; SI: severe infection.
CSI: clinical severe infection; pSBI: possible serious bacterial infection; SI: severe infection.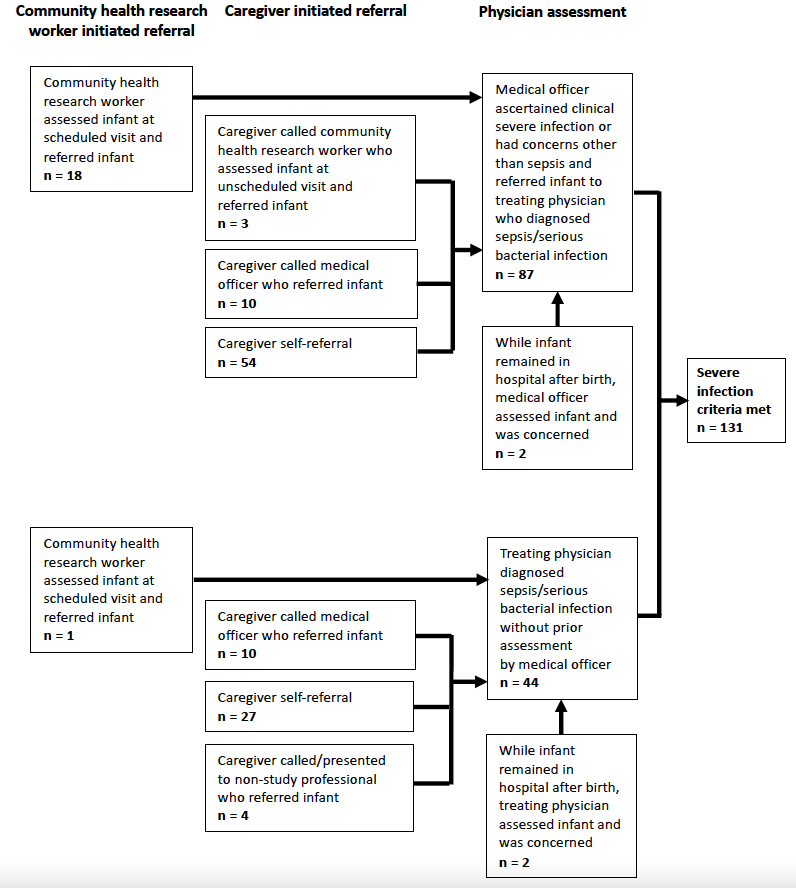 Note: Infants may have had multiple assessments by study and non-study personnel for a severe infection illness episode prior to meeting final severe infection criteria. Frequencies are based on initial presentation and assessment for the severe infection episode.a At least one sign of possible serious bacterial infection (poor feeding, convulsions, severe chest indrawing, fever (>=38oC), hypothermia ( <35.5oC), lethargy, or fast breathing (>=60 breaths per minute in infants <7 days old)) documented by a study medical officer and non-study treating physician decision to admit to hospital.CSI: clinical severe infection; pSBI: possible serious bacterial infection; SI: severe infection.Note: Infants may have had multiple assessments by study and non-study personnel for a severe infection illness episode prior to meeting final severe infection criteria. Frequencies are based on initial presentation and assessment for the severe infection episode.
Note: Infants may have had multiple assessments by study and non-study personnel for a severe infection illness episode prior to meeting final severe infection criteria. Frequencies are based on initial presentation and assessment for the severe infection episode.a At least one sign of possible serious bacterial infection (poor feeding, convulsions, severe chest indrawing, fever (>=38oC), hypothermia ( <35.5oC), lethargy, or fast breathing (>=60 breaths per minute in infants <7 days old)) documented by a study medical officer and non-study treating physician decision to admit to hospital.CSI: clinical severe infection; pSBI: possible serious bacterial infection; SI: severe infection.Note: Infants may have had multiple assessments by study and non-study personnel for a severe infection illness episode prior to meeting final severe infection criteria. Frequencies are based on initial presentation and assessment for the severe infection episode.