
Allergy, Immunology, and Rheumatology 2
Session: Allergy, Immunology, and Rheumatology 2

Sara E. Mertz, B.S.
Clinical Research Program Coordinator
Nationwide Children's Hospital
Columbus, Ohio, United States
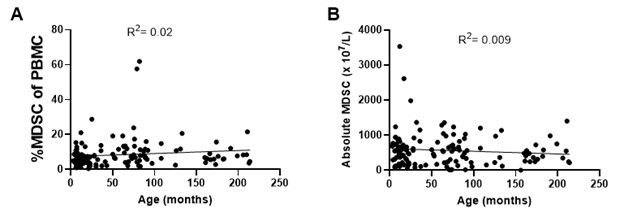 No differences were observed in the (A) percentages of MDSC of peripheral blood mononuclear cells (PBMC) or (B) absolute numbers of MDSC according to age.
No differences were observed in the (A) percentages of MDSC of peripheral blood mononuclear cells (PBMC) or (B) absolute numbers of MDSC according to age.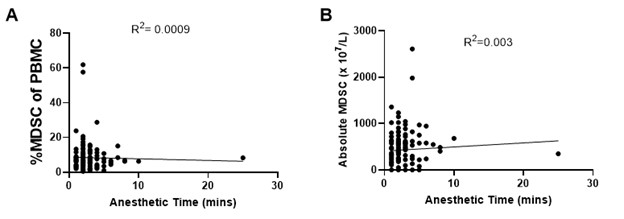 No association was observed in the (A) percentages of MDSC of PBMC or (B) absolute numbers of MDSC with increasing anesthetic time.
No association was observed in the (A) percentages of MDSC of PBMC or (B) absolute numbers of MDSC with increasing anesthetic time. 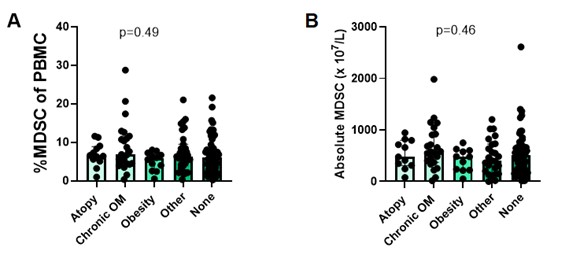 Children with history of atopy (n=12), chronic OM (n=24), obesity (n=10), or other comorbidities (n=28) had similar both (A) percentages MDSC of PBMC and (B) absolute MDSC compared to children without known comorbidities (n=63). OM= otitis media. No differences were observed in the (A) percentages of MDSC of peripheral blood mononuclear cells (PBMC) or (B) absolute numbers of MDSC according to age.No association was observed in the (A) percentages of MDSC of PBMC or (B) absolute numbers of MDSC with increasing anesthetic time. Children with history of atopy (n=12), chronic OM (n=24), obesity (n=10), or other comorbidities (n=28) had similar both (A) percentages MDSC of PBMC and (B) absolute MDSC compared to children without known comorbidities (n=63). OM= otitis media.
Children with history of atopy (n=12), chronic OM (n=24), obesity (n=10), or other comorbidities (n=28) had similar both (A) percentages MDSC of PBMC and (B) absolute MDSC compared to children without known comorbidities (n=63). OM= otitis media. No differences were observed in the (A) percentages of MDSC of peripheral blood mononuclear cells (PBMC) or (B) absolute numbers of MDSC according to age.No association was observed in the (A) percentages of MDSC of PBMC or (B) absolute numbers of MDSC with increasing anesthetic time. Children with history of atopy (n=12), chronic OM (n=24), obesity (n=10), or other comorbidities (n=28) had similar both (A) percentages MDSC of PBMC and (B) absolute MDSC compared to children without known comorbidities (n=63). OM= otitis media. 