
General Pediatrics 1
Session: General Pediatrics 1
 photo")
Nicole Heredia, Bachelor of Science (she/her/hers)
Clinical Research Assistant II
Boston Children's Hospital
Boston, Massachusetts, United States
.png) Immediate response rate is high; follow-up rates at 45 and 90 days show a decrease.
Immediate response rate is high; follow-up rates at 45 and 90 days show a decrease.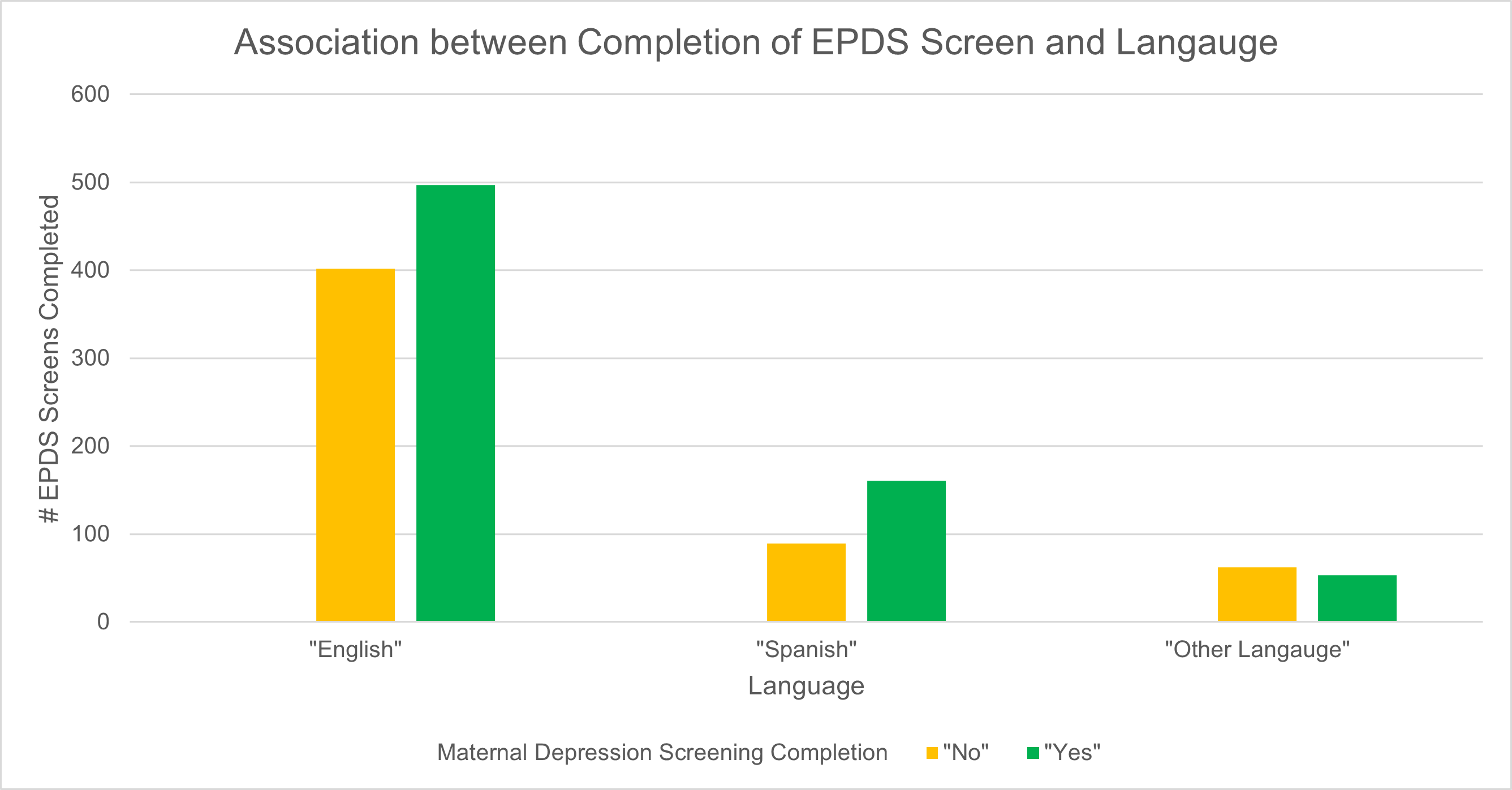 Screening completion rates for EPDS vary by language, with higher completion among Spanish-speaking mothers.Immediate response rate is high; follow-up rates at 45 and 90 days show a decrease.Screening completion rates for EPDS vary by language, with higher completion among Spanish-speaking mothers.
Screening completion rates for EPDS vary by language, with higher completion among Spanish-speaking mothers.Immediate response rate is high; follow-up rates at 45 and 90 days show a decrease.Screening completion rates for EPDS vary by language, with higher completion among Spanish-speaking mothers.