
Genomics/Epigenomics 1
Session: Genomics/Epigenomics 1
Anna-Thérèse Mehra, BA
Research Assistant
Boston Children's Hospital
New Canaan, Connecticut, United States
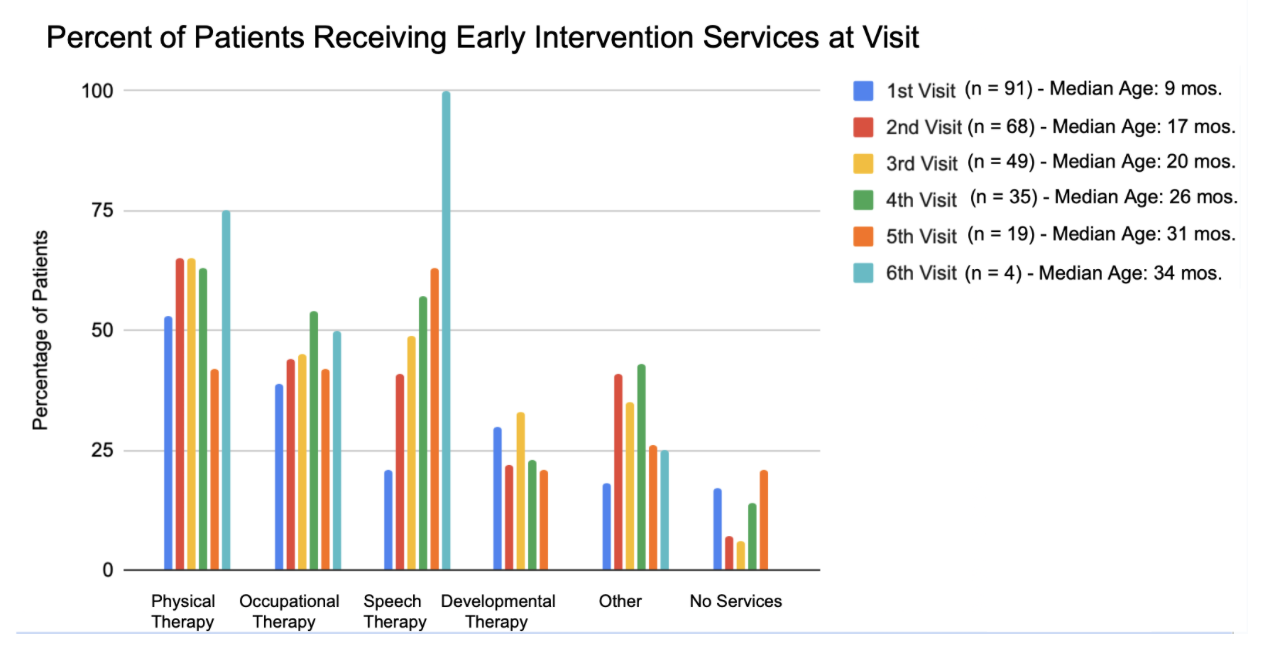 Percent of patients receiving Early Intervention services at each clinic visit
Percent of patients receiving Early Intervention services at each clinic visit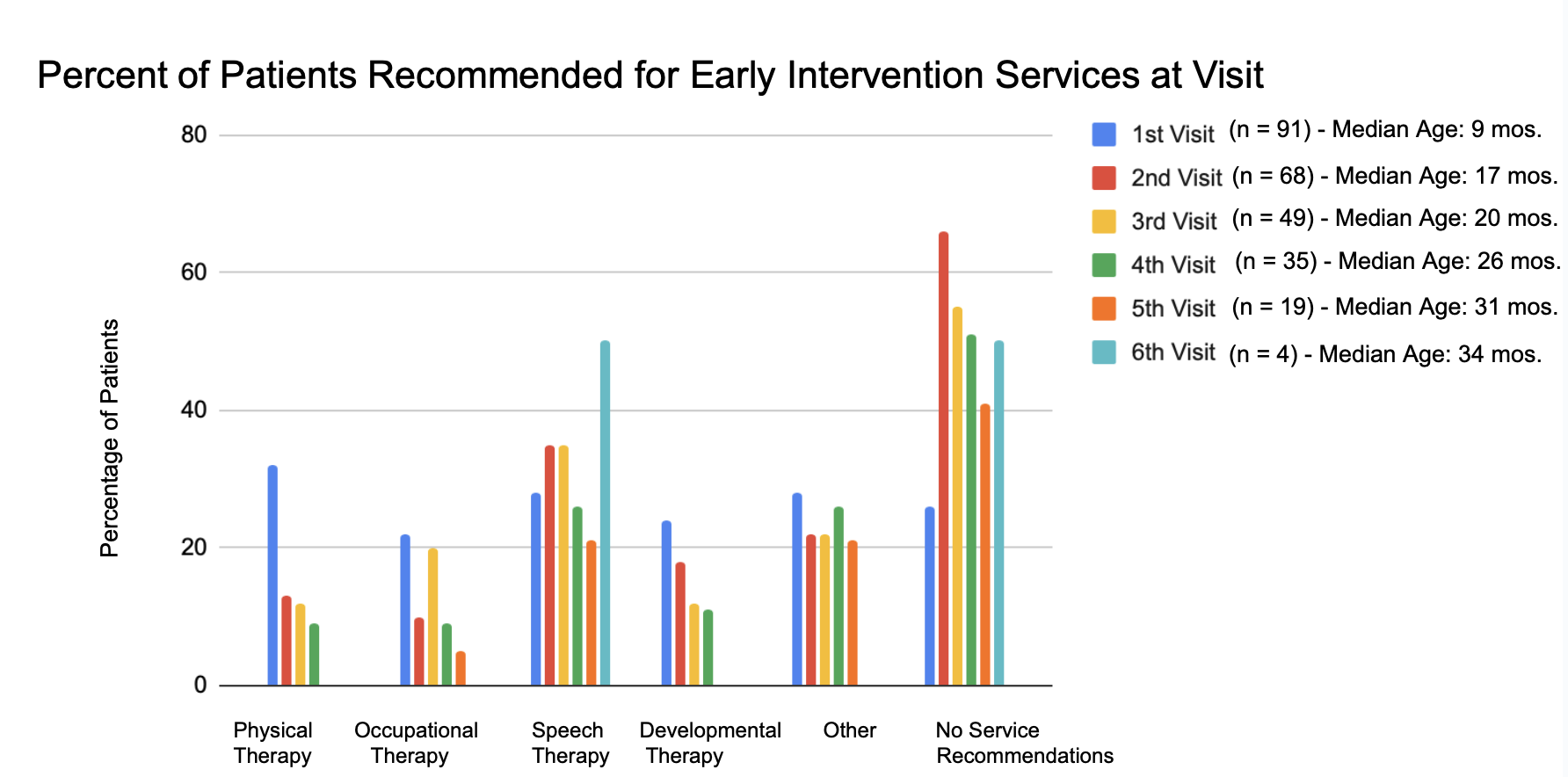 Percent of patients recommended for different Early Intervention services at each clinic visit
Percent of patients recommended for different Early Intervention services at each clinic visit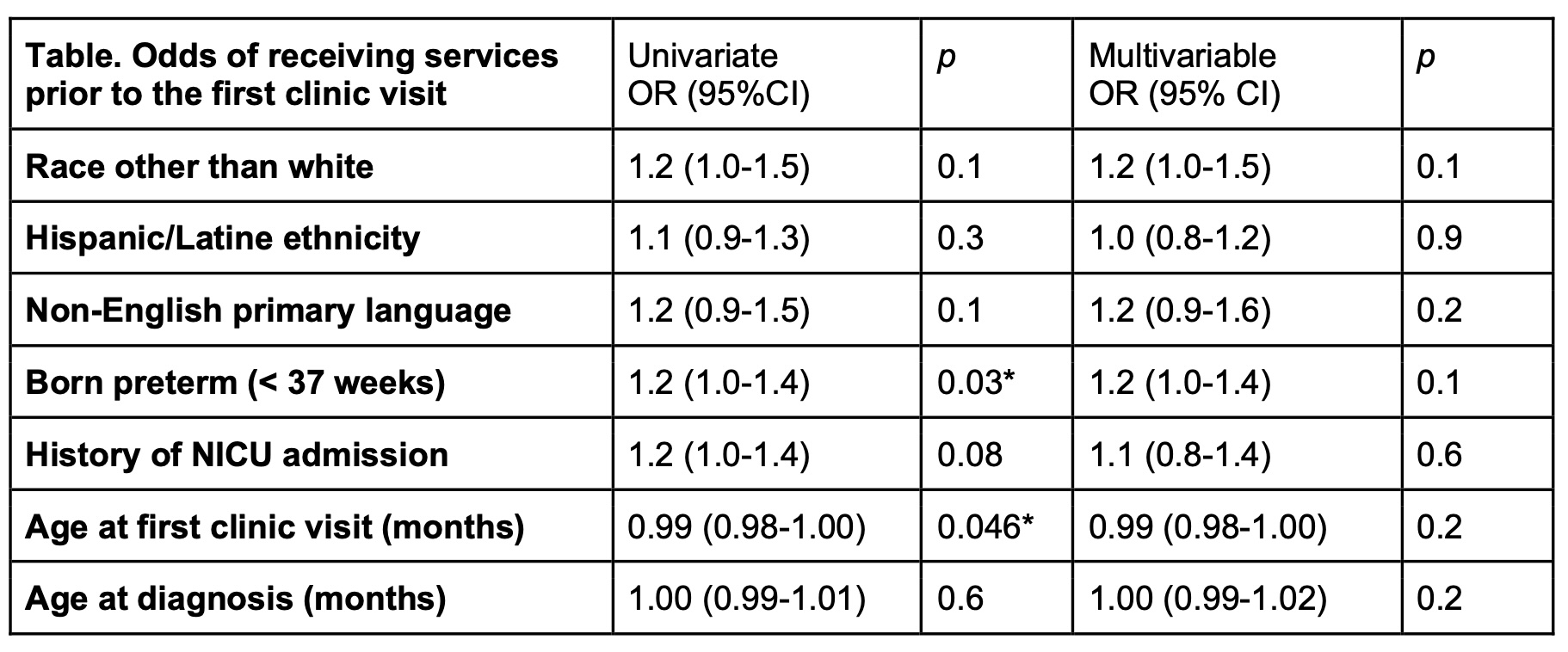 OR = odds ratio; CI = confidence interval.
OR = odds ratio; CI = confidence interval.