152 - Doppler echocardiography overestimates the systolic pressure of the right ventricle in pediatric patients with right ventricular pressure overload
Friday, April 25, 2025
5:30pm - 7:45pm HST
Publication Number: 152.4992
Manatomo Toyono, Akita University Graduate School of Medicine, Akita, Akita, Japan; Miho Hatakeyama-Sasaki, Akita University Graduate School of Medicine, Akita, Akita, Japan; Yuichi Nakamoto, Akita University Graduate School of Medicine, Akita, Akita, Japan
Associate Professor Akita University Graduate School of Medicine Akita, Akita, Japan
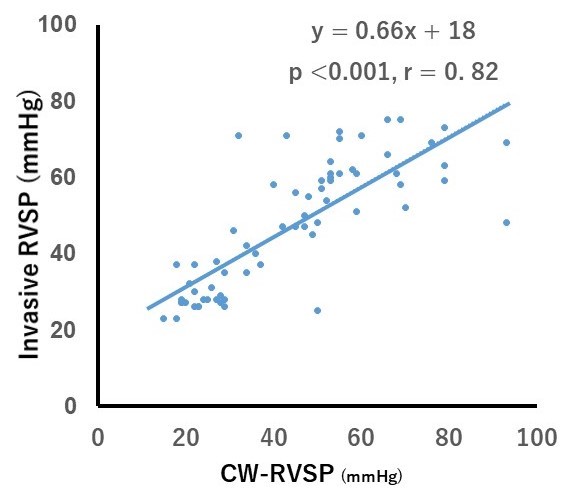
Background: The standard method for measuring right ventricular systolic pressure (RVSP) is right heart catheterization, but due to its invasiveness, it cannot be used for routine follow-up in pediatric patients. When tricuspid regurgitation (TR) is present, the maximum velocity can be measured using continuous wave (CW) Doppler and the modified Bernoulli equation can be applied to obtain an approximate estimate of the systolic TR pressure gradient. However, there are only a limited number of studies that have examined the accuracy of the CW-RVSP method and the invasive RVSP method. Objective: The objective of this study is to determine whether the CW-RVSP method is an accurate assessment of the invasive RVSP method. Design/Methods: A prospective study was conducted on sixty-six patients (age: 0.2-12 years, median 1.4 years; female, 62%) who underwent noninvasive and invasive RVSP measurements simultaneously. The indications for invasive testing were congenital heart disease in fifty-four cases and idiopathic pulmonary arterial hypertension in twelve cases. CW-RVSP was calculated as the sum of the right atrial pressure and the peak pressure gradient estimated by the modified Bernoulli equation. Right atrial pressure was estimated from the diameter of the inferior vena cava and its changes with respiration, as well as from the blood flow profile of the hepatic vein. Results: The minimum, maximum, and median invasive RVSPs were 23, 75, and 47.5 mmHg, respectively. CW-RVSP showed a significant linear correlation with invasively measured RVSP (p < 0.001, r = 0.82, Figure 1). The relative error, i.e., the ratio of the difference between CW-RVSP and invasive RVSP to the mean of CW-RVSP and invasive RVSP, ranged from -76% to 67% (median 11%). CW-RVSP showed a significant linear correlation with relative error (p < 0.001; r = 0.63; Figure 2). When CW-RVSP exceeded 60 mmHg, the greater the CW-RVSP, the greater the overestimation of invasive RVSP.
Conclusion(s): This study shows that CW-Doppler may overestimate RVSP in pediatric patients with right ventricular pressure overload.
Figure 1 Relationship between CW-RVSP and invasive RVSP

 photo")
 Relationship between CW-RVSP and invasive RVSP
Relationship between CW-RVSP and invasive RVSP.jpg) Relative error of CW-RVSP
Relative error of CW-RVSP