
Neonatal Quality Improvement 1
Session: Neonatal Quality Improvement 1
 Credit")
 photo")
Emma Harding, MD (she/her/hers)
Fellow
University of Colorado School of Medicine
Denver, Colorado, United States
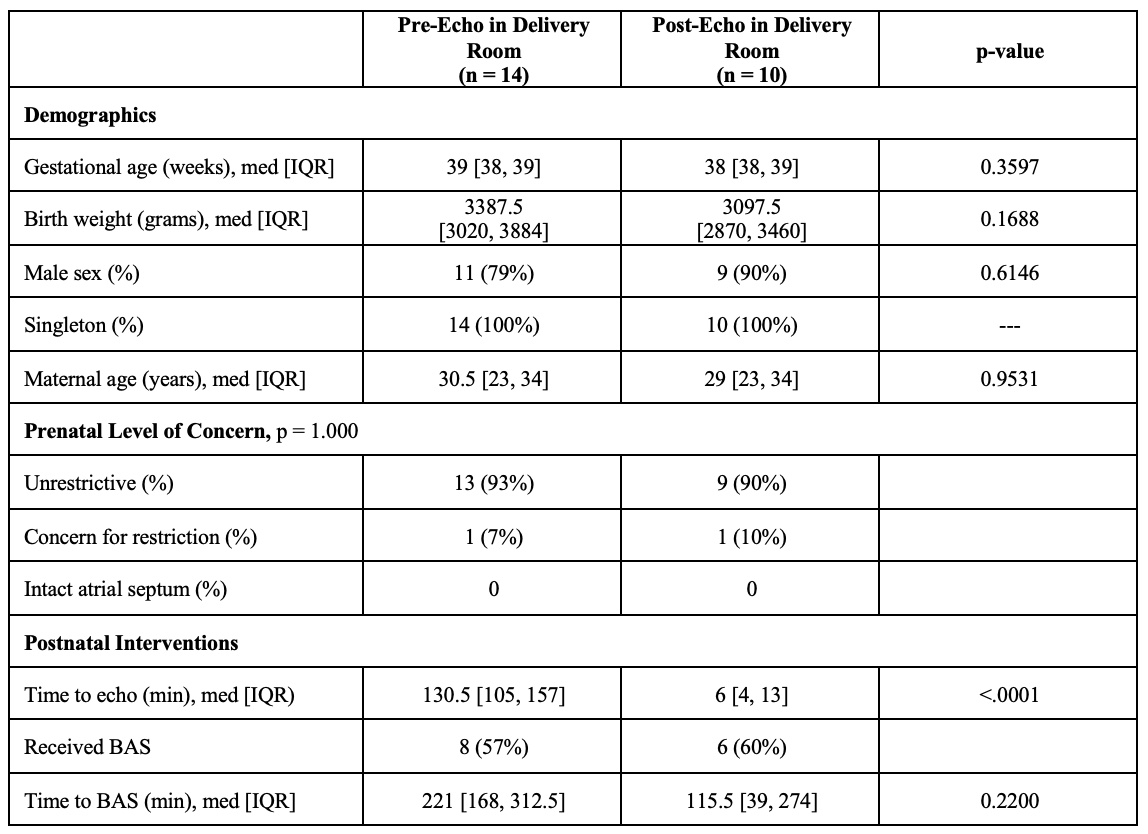
 Control chart of time to first postnatal echo
Control chart of time to first postnatal echo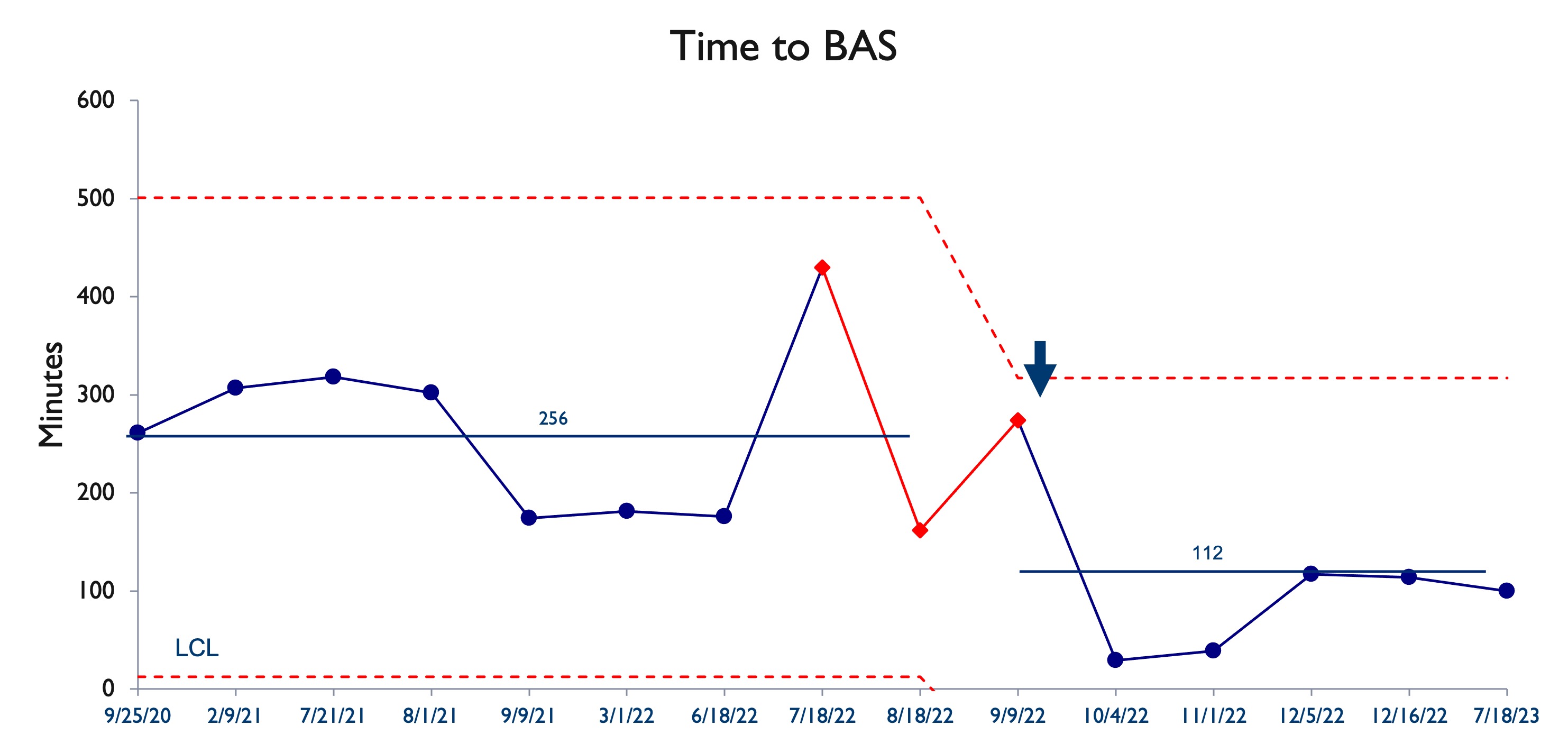 Control chart of time to balloon atrial septostomy
Control chart of time to balloon atrial septostomy