General Pediatrics 2
Session: General Pediatrics 2
 Credit")
 photo")
Gabrielle E. Sanatani, MB, BCh, BAO (she/her/hers)
Resident
Children's Hospital Colorado
Denver, Colorado, United States
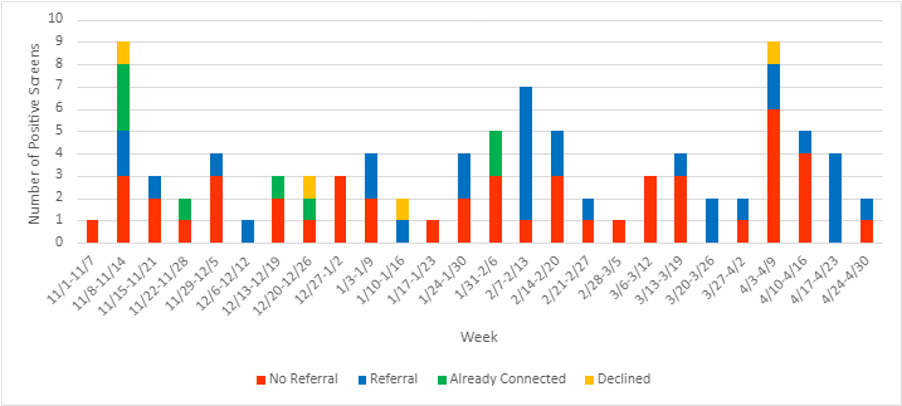
.png) 1: Discussion with clerks to improve screening handout at front desk. 2: Screening champion present in clinic daily for entire month. 3: Reminder email sent to clerks and staff. 4: Discussion with clerks, reminder email sent. 5: Reminder email sent, verbal reminders during daily huddle meetings. 6: Screening champion monitoring schedule.
1: Discussion with clerks to improve screening handout at front desk. 2: Screening champion present in clinic daily for entire month. 3: Reminder email sent to clerks and staff. 4: Discussion with clerks, reminder email sent. 5: Reminder email sent, verbal reminders during daily huddle meetings. 6: Screening champion monitoring schedule.