
Neonatal Quality Improvement 3
Session: Neonatal Quality Improvement 3
 Credit")
 photo")
Rebecca Sherlock, MD (she/her/hers)
Neonatologist
other
Whistler, British Columbia, Canada
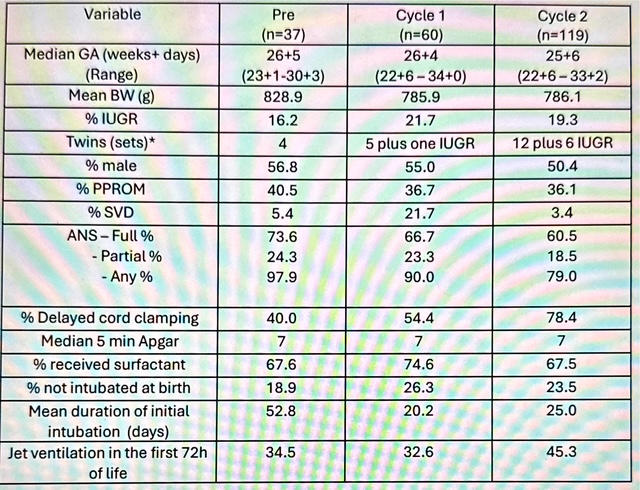 *Number reported reflects full sets of twins plus infants of twin pairs meeting criteria for inclusion in the Tiny Baby Initiative.
*Number reported reflects full sets of twins plus infants of twin pairs meeting criteria for inclusion in the Tiny Baby Initiative. 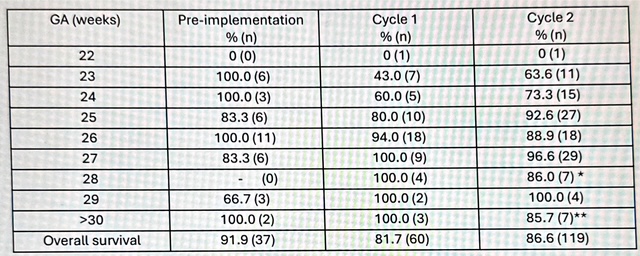 *the one infant that died in this was 600g severely growth restricted
*the one infant that died in this was 600g severely growth restricted 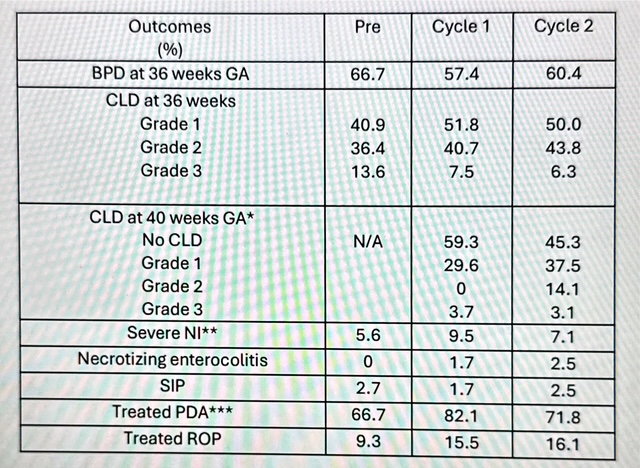 *of those that had CLD at 36 weeks GA
*of those that had CLD at 36 weeks GA 