
Global Neonatal & Children's Health 2
Session: Global Neonatal & Children's Health 2
 photo")
Marisa Cristin Woo, MS (she/her/hers)
Medical student
University of Hawaii, John A. Burns School of Medicine
San Jose, California, United States
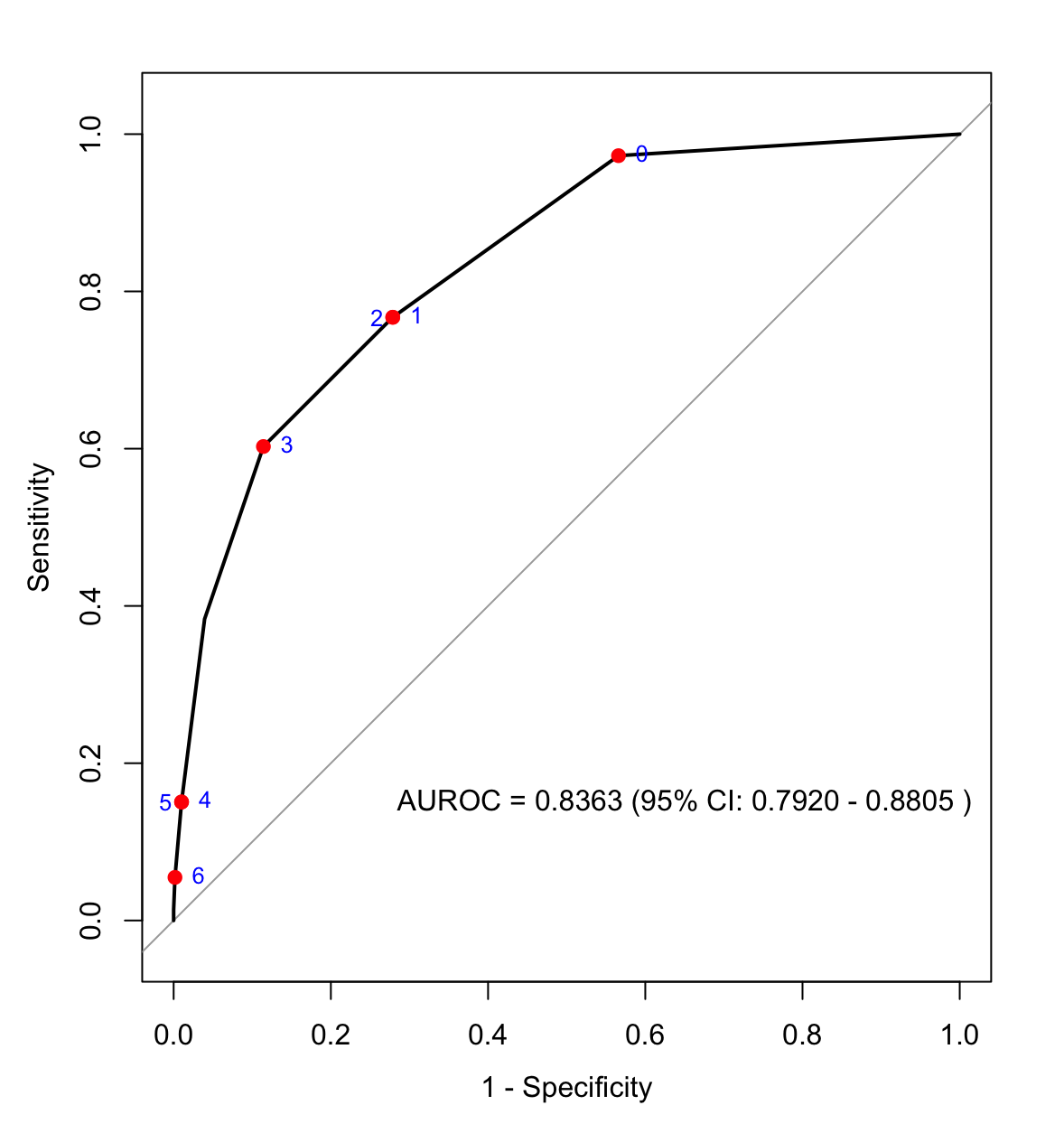 Figure 1: The receiver operating characteristic (ROC) curve shows the discriminative ability of the Pediatric Early Warning Score for Resource-Limited Settings (PEWS-RL) to identify clinical deterioration events (CDE) in the day following hospital presentation due to an acute illness or injury. The area under the ROC (AUROC) was 0.8363 [95% confidence interval, 0.7920-0.8805]. A PEWS-RL score ≥3 had a sensitivity of 60.3% and specificity of 88.6% to predict CDE.
Figure 1: The receiver operating characteristic (ROC) curve shows the discriminative ability of the Pediatric Early Warning Score for Resource-Limited Settings (PEWS-RL) to identify clinical deterioration events (CDE) in the day following hospital presentation due to an acute illness or injury. The area under the ROC (AUROC) was 0.8363 [95% confidence interval, 0.7920-0.8805]. A PEWS-RL score ≥3 had a sensitivity of 60.3% and specificity of 88.6% to predict CDE.