
Cardiology 3
Session: Cardiology 3
 photo")
Jenil M. Rana, OMS-II (he/him/his)
Medical Student
University of North Texas Health Science Center
North Richland Hills, Texas, United States
.png) Comparison of Normal testing group to Abnormal testing group. P-value < 0.05 considered statistically significant, marked in bold font.
Comparison of Normal testing group to Abnormal testing group. P-value < 0.05 considered statistically significant, marked in bold font. 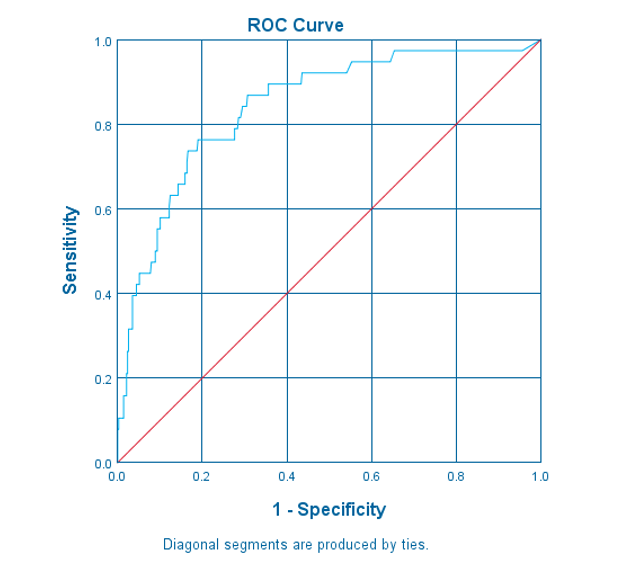 Receiver operating characteristic analysis of troponin levels at ER presentation for associated abnormal cardiac testing.
Receiver operating characteristic analysis of troponin levels at ER presentation for associated abnormal cardiac testing.