
General Pediatrics 2
Session: General Pediatrics 2
 photo")
India Gill, MPH, PhD (she/her/hers)
Postdoctoral Fellow
University of California, San Francisco, School of Medicine
San Francisco, California, United States
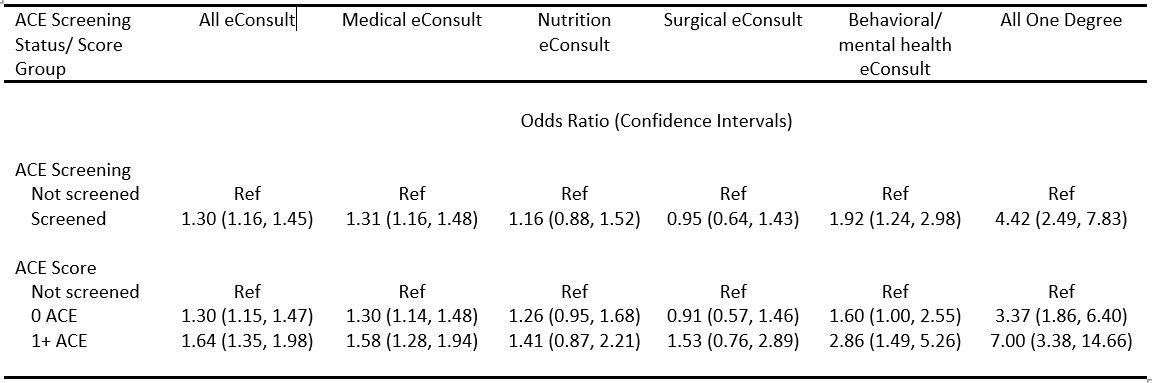 Reference group is non-screened pediatric patients. Patients were propensity score matched on age, gender, clinic, insurance, appointment type, number of primary care visits, and primary care visit date quartile. Outcome models were further adjusted for covariates with standardized mean differences exceeding 0.2.
Reference group is non-screened pediatric patients. Patients were propensity score matched on age, gender, clinic, insurance, appointment type, number of primary care visits, and primary care visit date quartile. Outcome models were further adjusted for covariates with standardized mean differences exceeding 0.2.