
Cardiology 2
Session: Cardiology 2
 photo")
Carissa M. BakerSmith, MD MPH (she/her/hers)
Director of Pediatric Preventive Cardiology
Nemours Children's Hospital
Ellicott City, Maryland, United States
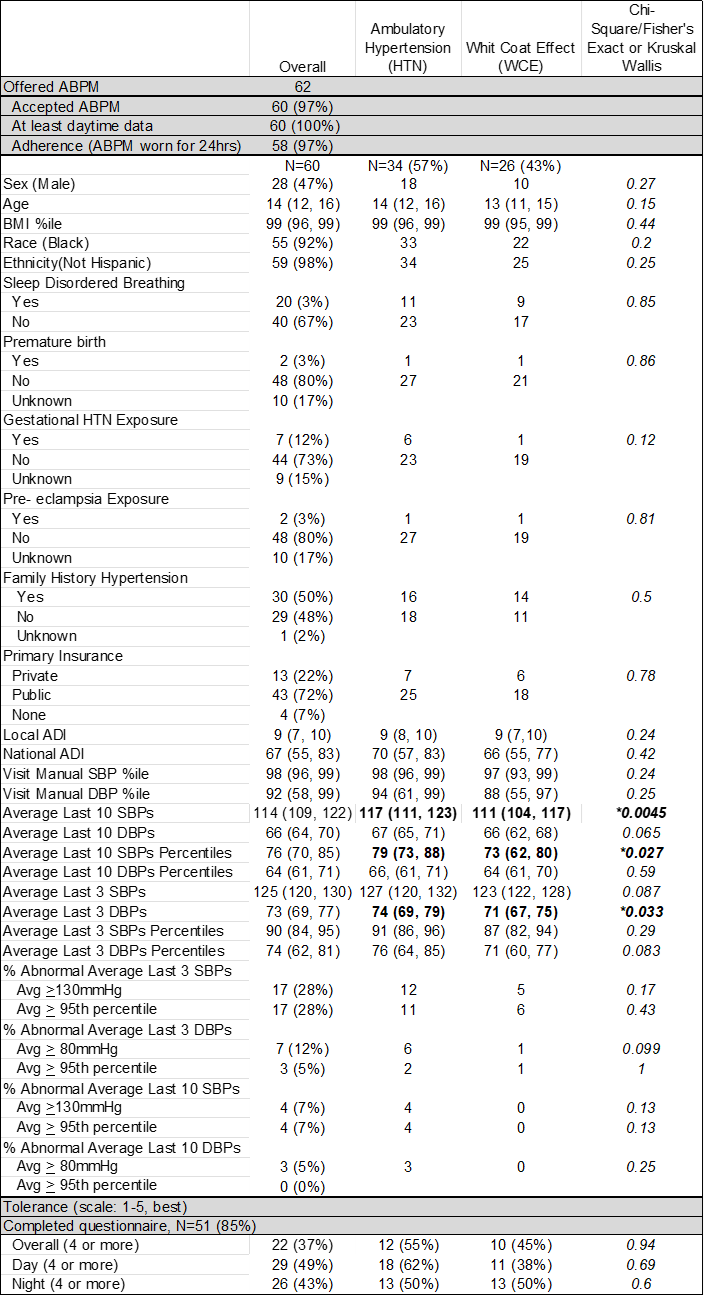 Tolerance of ABPM was assessed according to a Likert scale (1 to 5, 5=well tolerated).
Tolerance of ABPM was assessed according to a Likert scale (1 to 5, 5=well tolerated). Tolerance of ABPM was assessed according to a Likert scale (1 to 5, 5=well tolerated).
Tolerance of ABPM was assessed according to a Likert scale (1 to 5, 5=well tolerated).