
Pulmonology
Session: Pulmonology
 photo")
Meghan E. McGarry, MD, MAS, ATSF (she/her/hers)
Associate Professor of Pediatrics
University of Washington School of Medicine
Seattle, Washington, United States
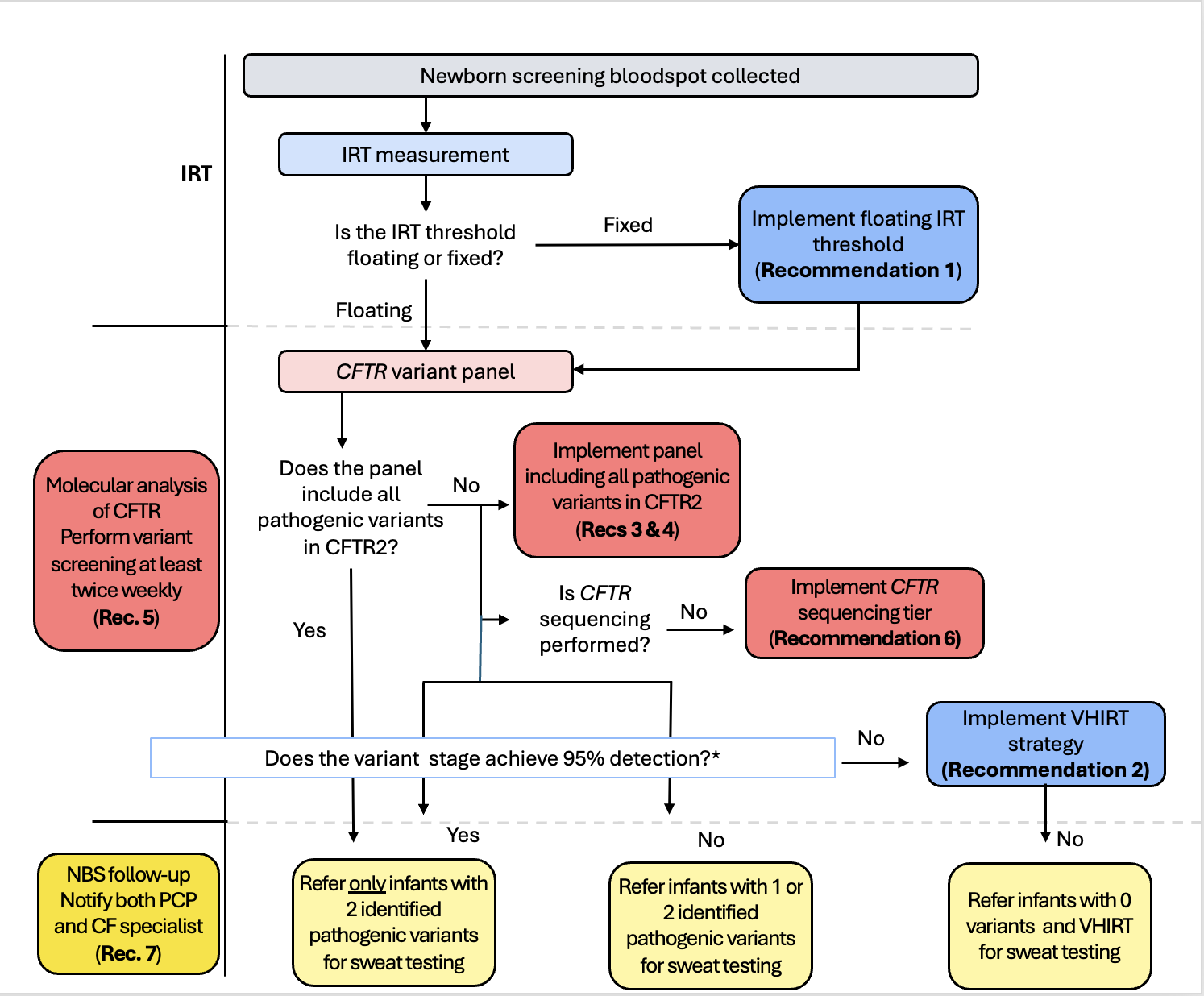 Flowchart of ideal CF NBS algorithm and decision points for implementing change
Flowchart of ideal CF NBS algorithm and decision points for implementing change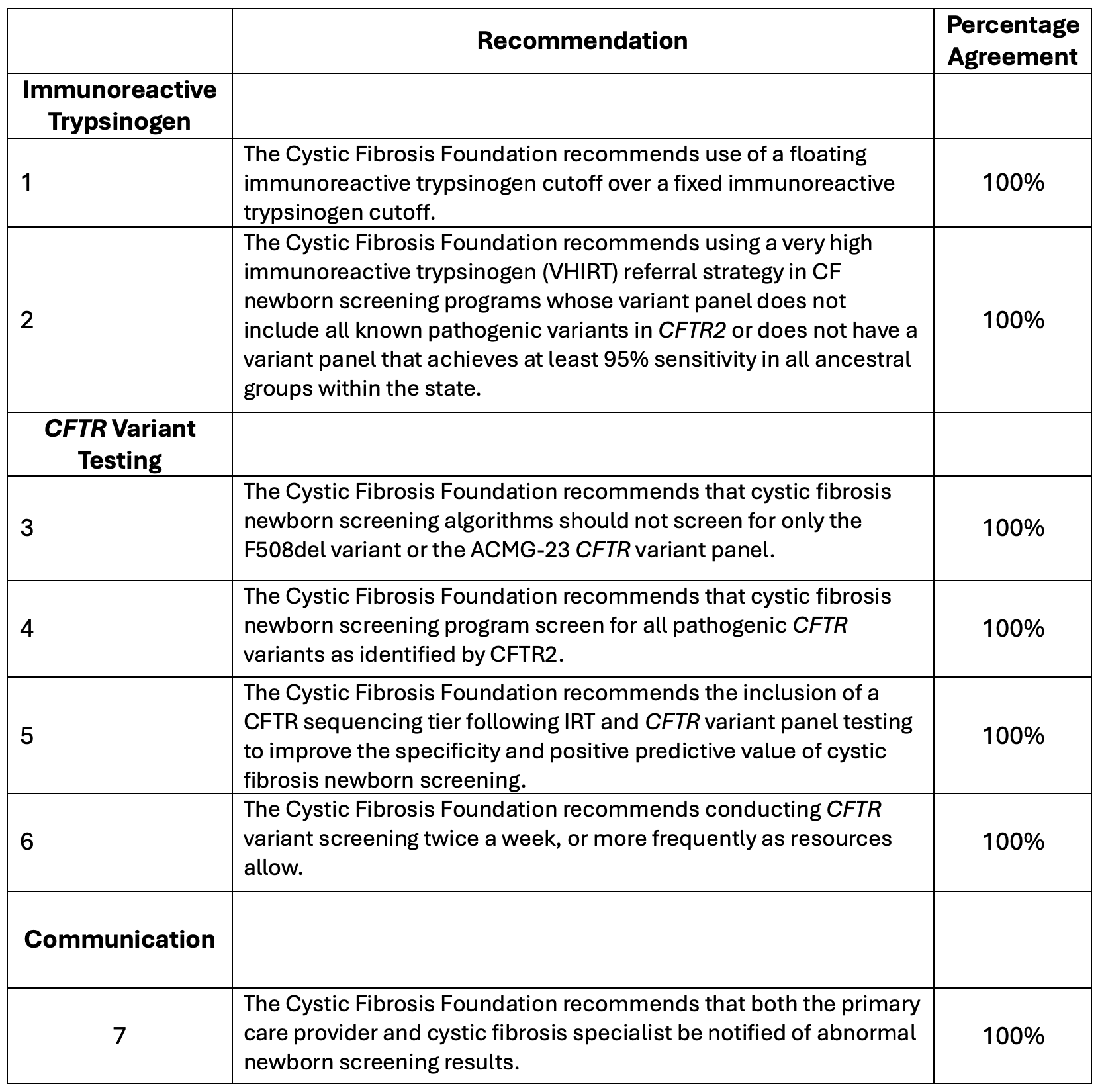 Consensus Recommendation Statements for Cystic Fibrosis Newborn Screening
Consensus Recommendation Statements for Cystic Fibrosis Newborn Screening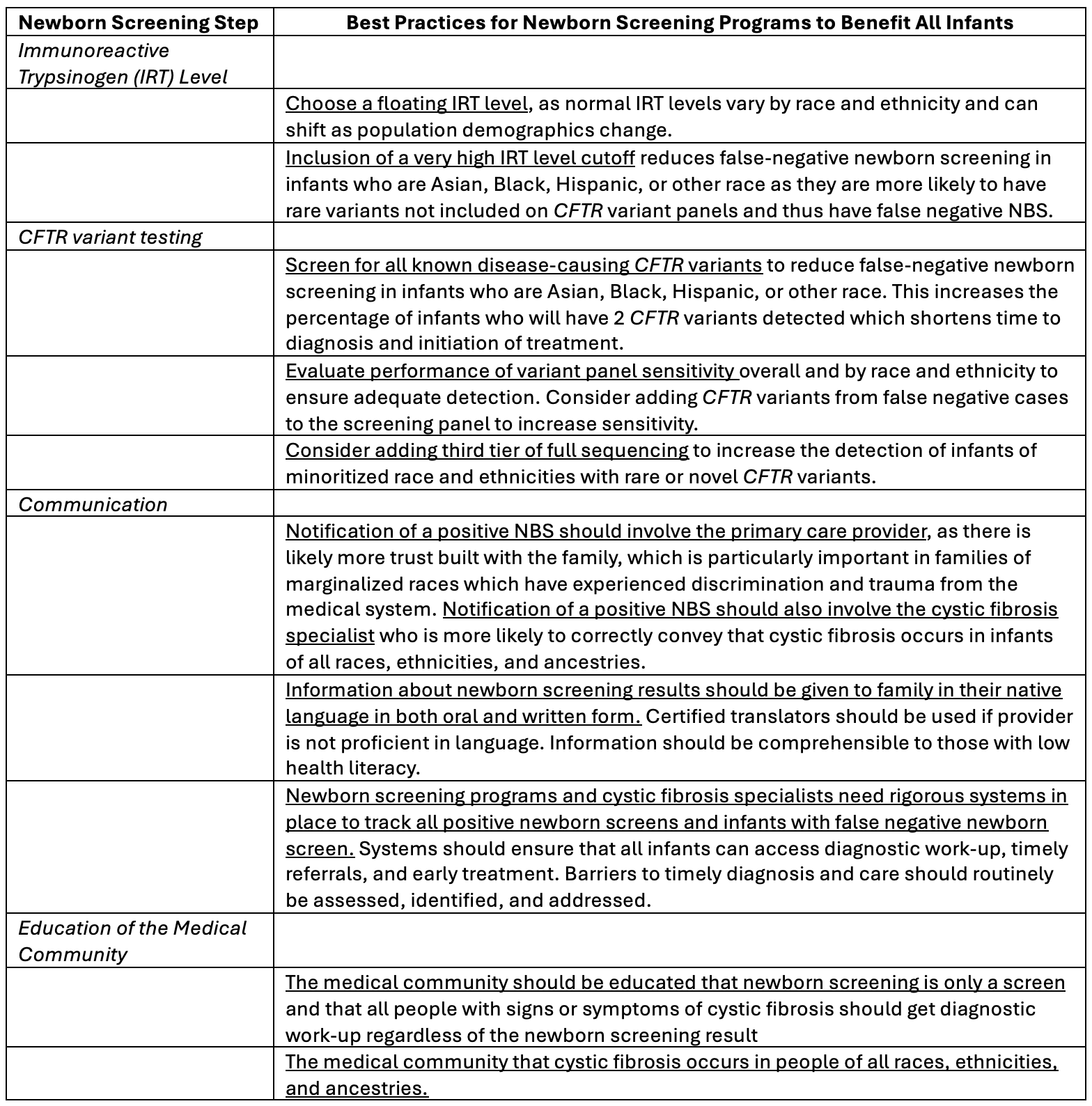 Considerations for Equity in Cystic Fibrosis Newborn Screening
Considerations for Equity in Cystic Fibrosis Newborn Screening