
Neonatal General 4: Novel Technology and Therapies
Session: Neonatal General 4: Novel Technology and Therapies
 photo")
Ha L. Tran, MD (she/her/hers)
NICU Fellow
Nemours Alfred I. duPont Hospital for Children
PHILADELPHIA, Pennsylvania, United States
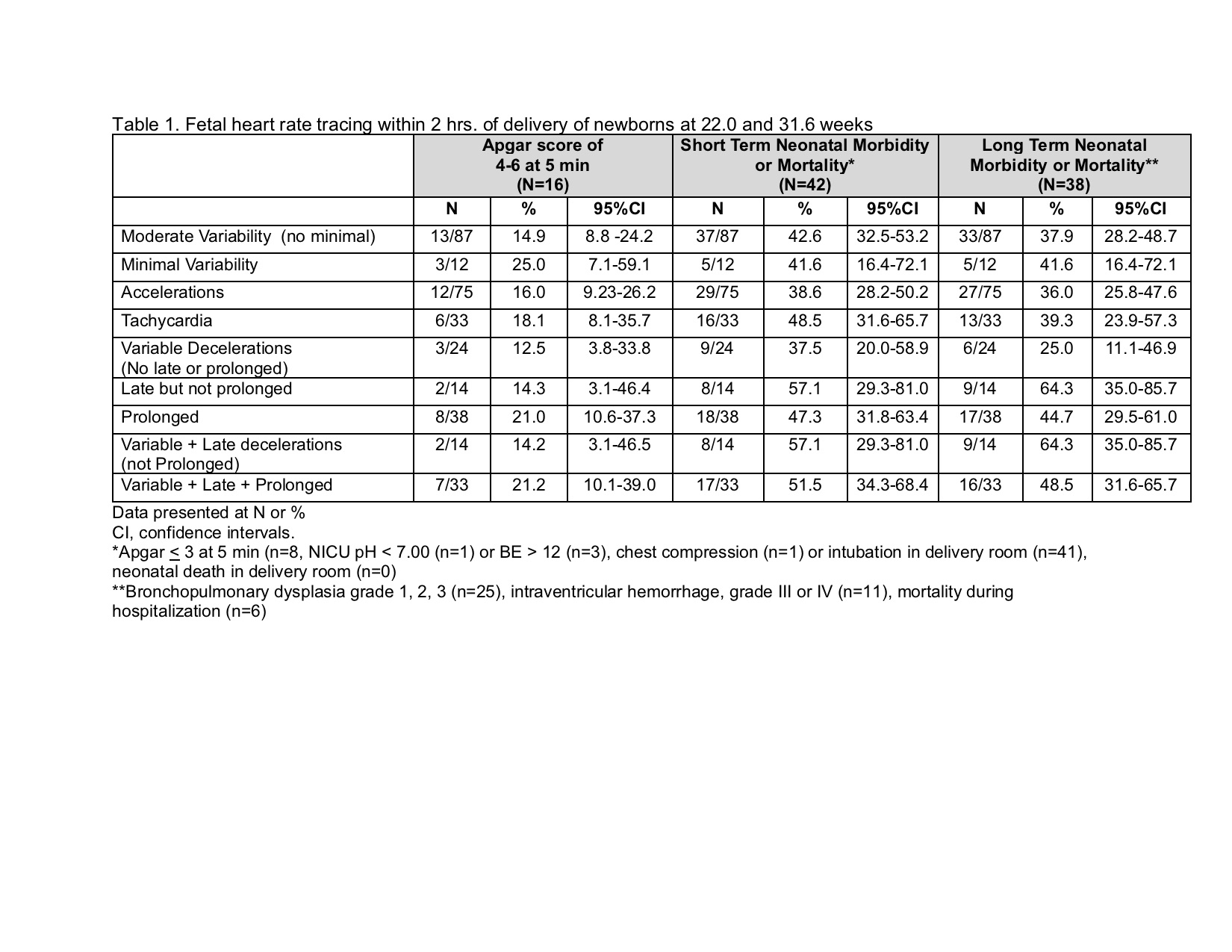 Fetal heart rate tracing within 2 hrs of delivery of newborns at 22.0 and 31.6 weeks
Fetal heart rate tracing within 2 hrs of delivery of newborns at 22.0 and 31.6 weeks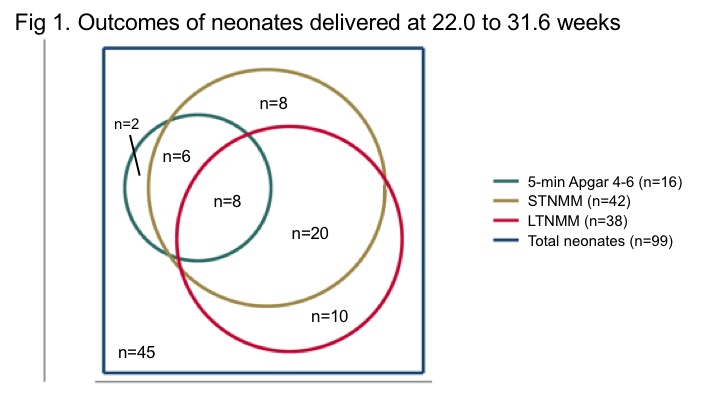 Outcomes of neonates delivered at 22.0 to 31.6 weeks
Outcomes of neonates delivered at 22.0 to 31.6 weeks