
Infectious Diseases 2: Bacterial infections
Session: Infectious Diseases 2: Bacterial infections
 photo")
Ami J. Patel, MD (she/her/hers)
Clinical Fellow
Columbia University Vagelos College of Physicians and Surgeons
New York, New York, United States
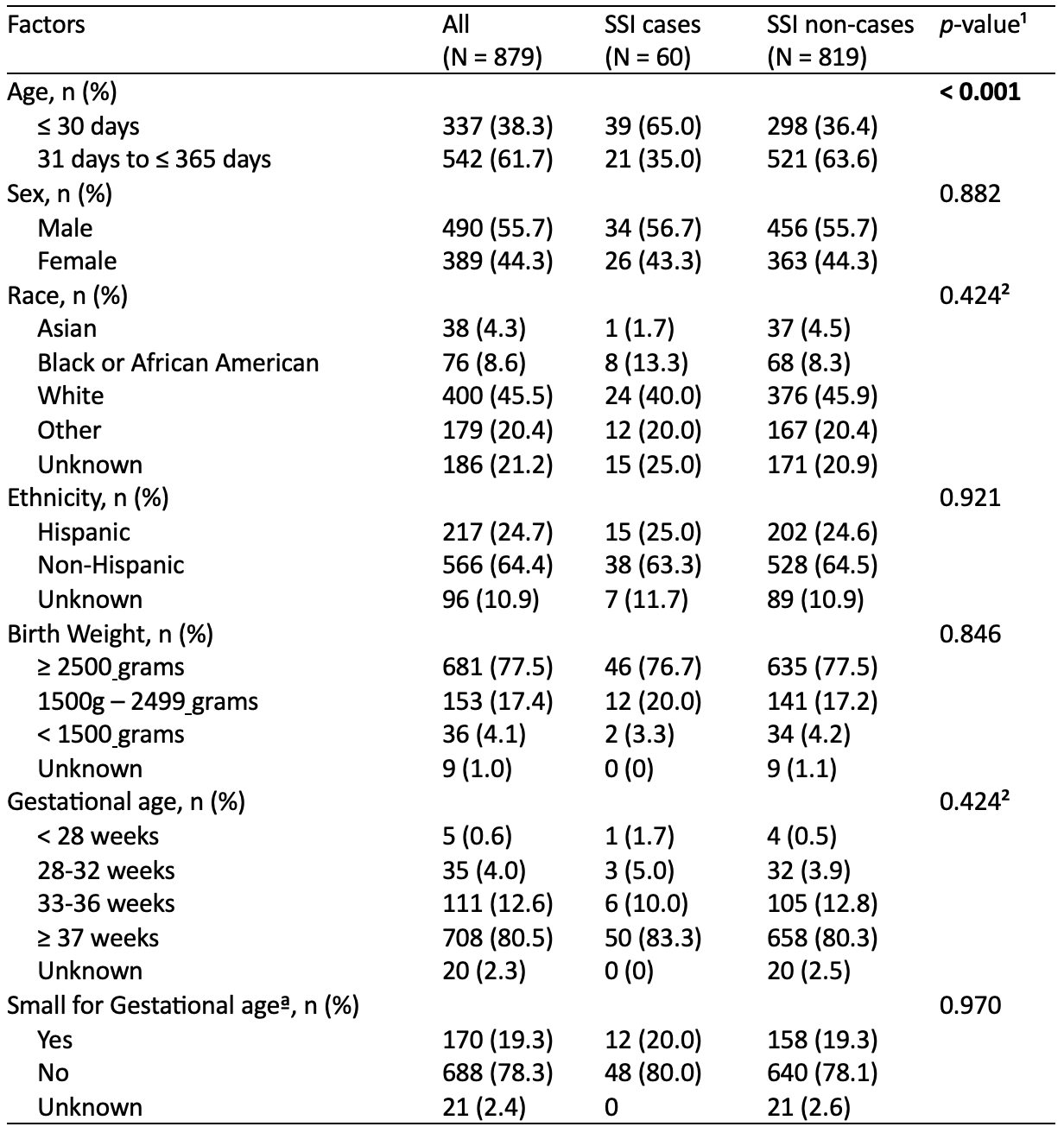 ¹p-value for χ² test statistic comparing cases vs non-cases; p-value < 0.05 was used for significance, unknown values not included
¹p-value for χ² test statistic comparing cases vs non-cases; p-value < 0.05 was used for significance, unknown values not included 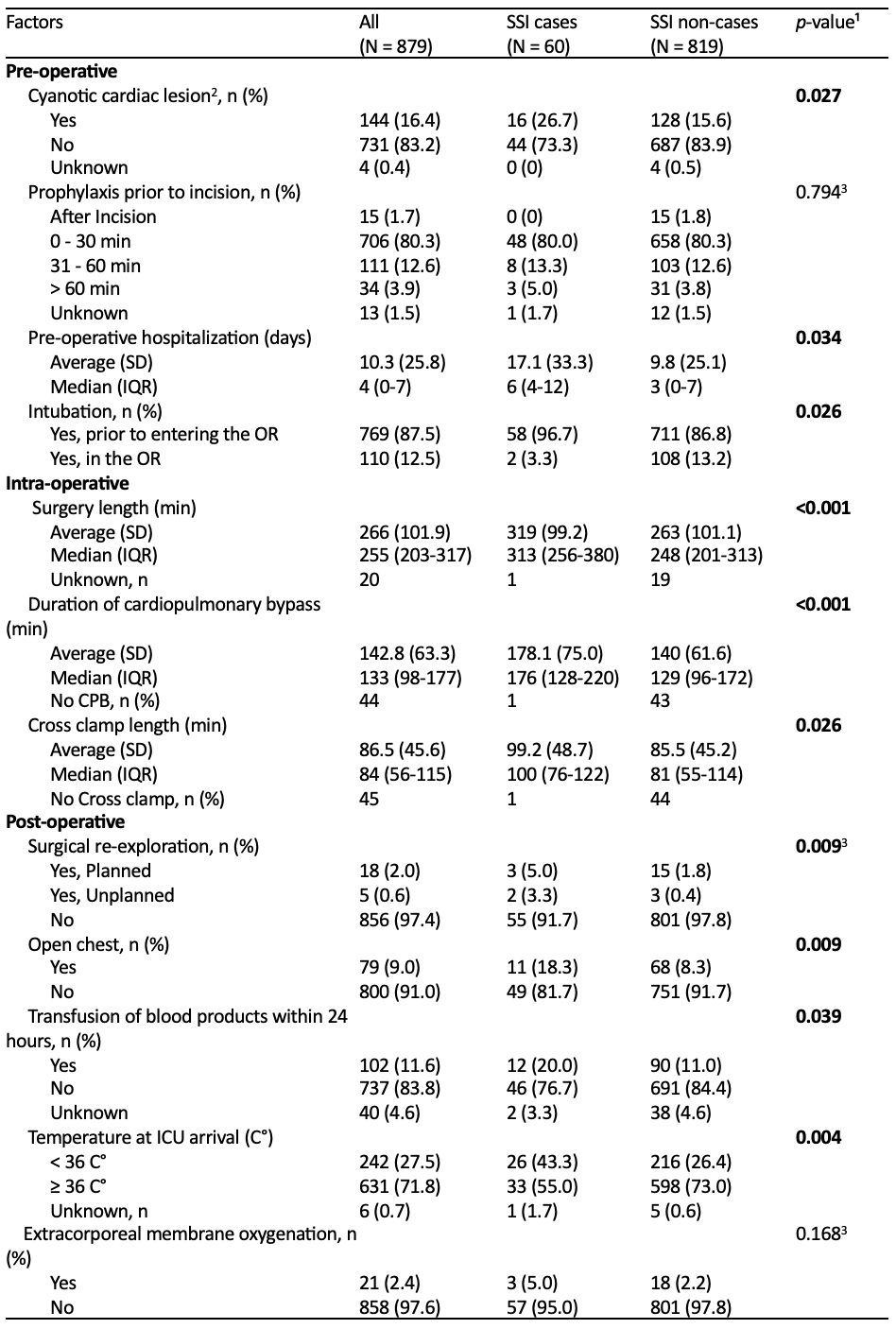 ¹p-value for χ² test statistic or 2-tailed t-test comparing cases vs non-cases; p-value < 0.05 was used for significance, unknown not included ¹p-value for χ² test statistic comparing cases vs non-cases; p-value < 0.05 was used for significance, unknown values not included ¹p-value for χ² test statistic or 2-tailed t-test comparing cases vs non-cases; p-value < 0.05 was used for significance, unknown not included
¹p-value for χ² test statistic or 2-tailed t-test comparing cases vs non-cases; p-value < 0.05 was used for significance, unknown not included ¹p-value for χ² test statistic comparing cases vs non-cases; p-value < 0.05 was used for significance, unknown values not included ¹p-value for χ² test statistic or 2-tailed t-test comparing cases vs non-cases; p-value < 0.05 was used for significance, unknown not included 