
Global Neonatal & Children's Health 1
Session: Global Neonatal & Children's Health 1

Alastair Fung, MD, MPH
Clinical Fellow
The Hospital for Sick Children
Toronto, Ontario, Canada
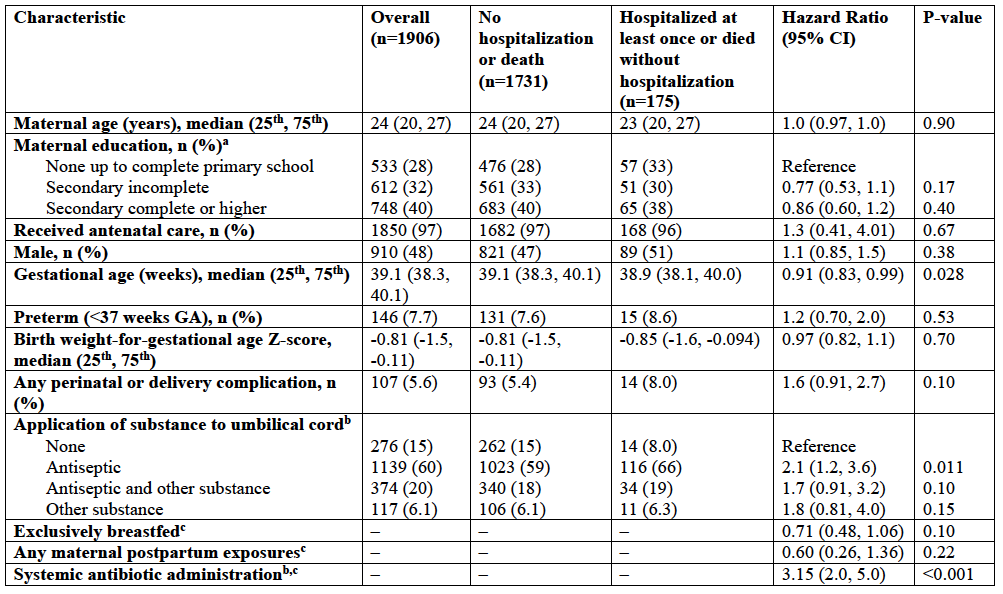 a Denominator is the number of mothers (n=1893).
a Denominator is the number of mothers (n=1893).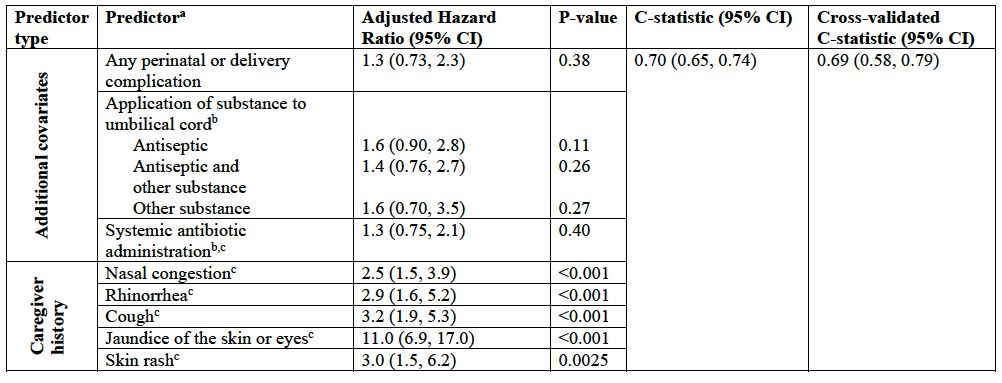 a Predictors from caregiver history selected using backward selection based on threshold p-value of <0.2. Additional covariates included as predictors based on clinical judgment and if they improved model performance (C-statistic).
a Predictors from caregiver history selected using backward selection based on threshold p-value of <0.2. Additional covariates included as predictors based on clinical judgment and if they improved model performance (C-statistic).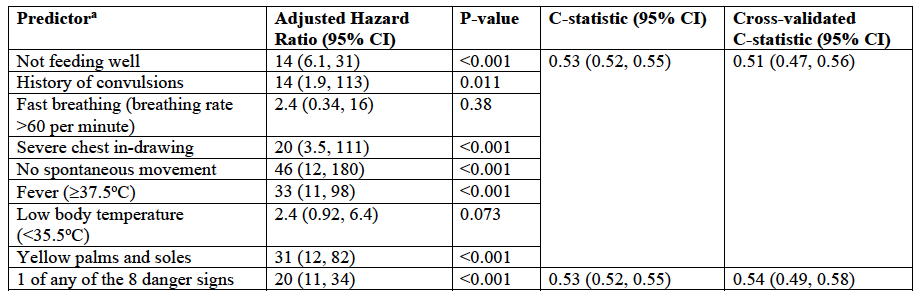 a Observation window for predictors: In the last 7 days including the day of the home visit or since the last home visit (whichever is most recent).a Denominator is the number of mothers (n=1893).a Predictors from caregiver history selected using backward selection based on threshold p-value of <0.2. Additional covariates included as predictors based on clinical judgment and if they improved model performance (C-statistic).a Observation window for predictors: In the last 7 days including the day of the home visit or since the last home visit (whichever is most recent).
a Observation window for predictors: In the last 7 days including the day of the home visit or since the last home visit (whichever is most recent).a Denominator is the number of mothers (n=1893).a Predictors from caregiver history selected using backward selection based on threshold p-value of <0.2. Additional covariates included as predictors based on clinical judgment and if they improved model performance (C-statistic).a Observation window for predictors: In the last 7 days including the day of the home visit or since the last home visit (whichever is most recent).