
Immunizations/Delivery 1
Session: Immunizations/Delivery 1
 photo")
Ziyi Wang, MS (she/her/hers)
Statistician
Children’s Hospital of Philadelphia
Exton, Pennsylvania, United States
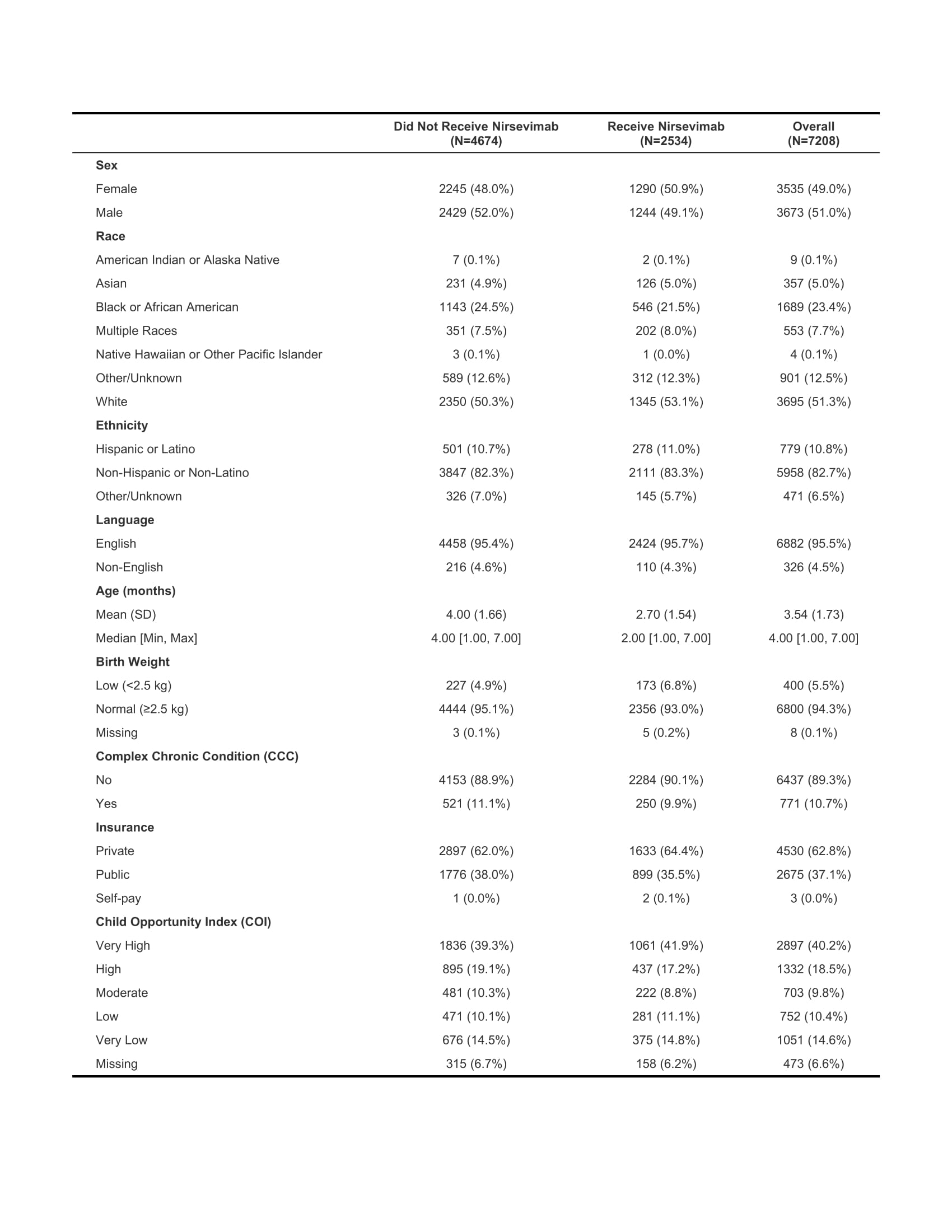 All children across 32 CHOP primary care practices eligible for nirsevimab in the 2023-2024 RSV season
All children across 32 CHOP primary care practices eligible for nirsevimab in the 2023-2024 RSV season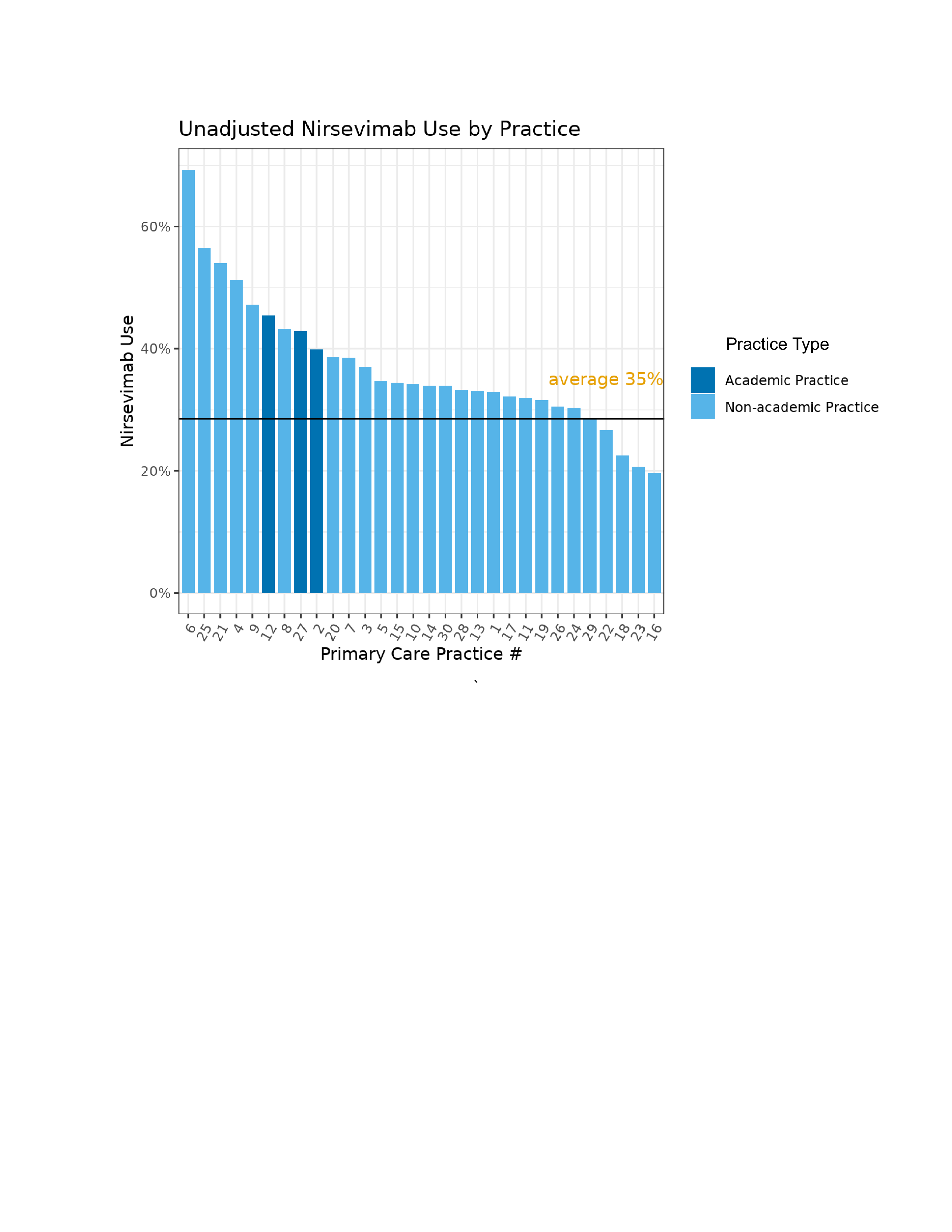 Practice #18 includes three different practices as they share the same group of clinicians
Practice #18 includes three different practices as they share the same group of clinicians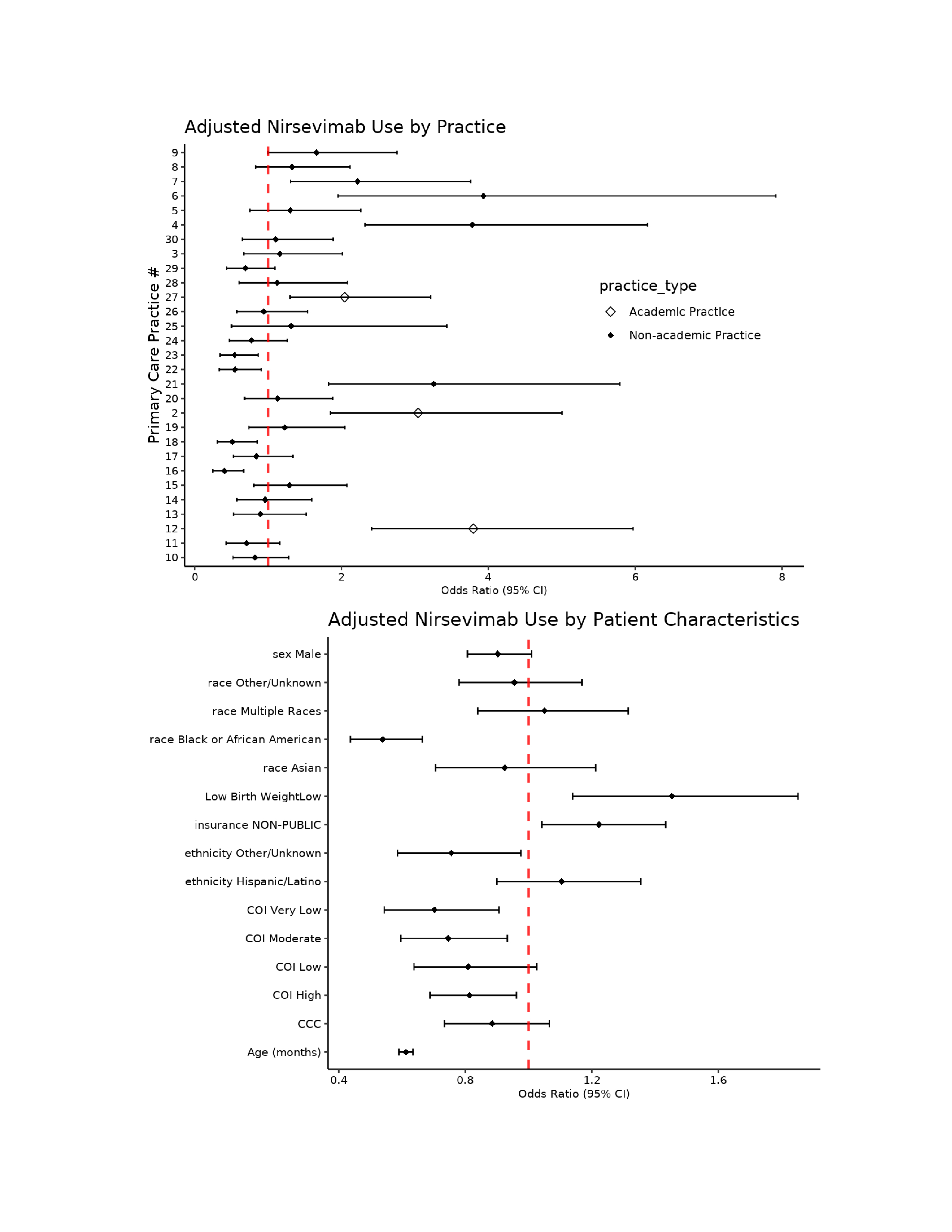 Top: Reference group: practice #1
Top: Reference group: practice #1