
Neonatal General 1: Respiratory, BPD
Session: Neonatal General 1: Respiratory, BPD
 photo")
Thomas Davis, MD (he/him/his)
Pediatric Resident
Childrens Hospital of Philadelphia
Philadelphia, Pennsylvania, United States
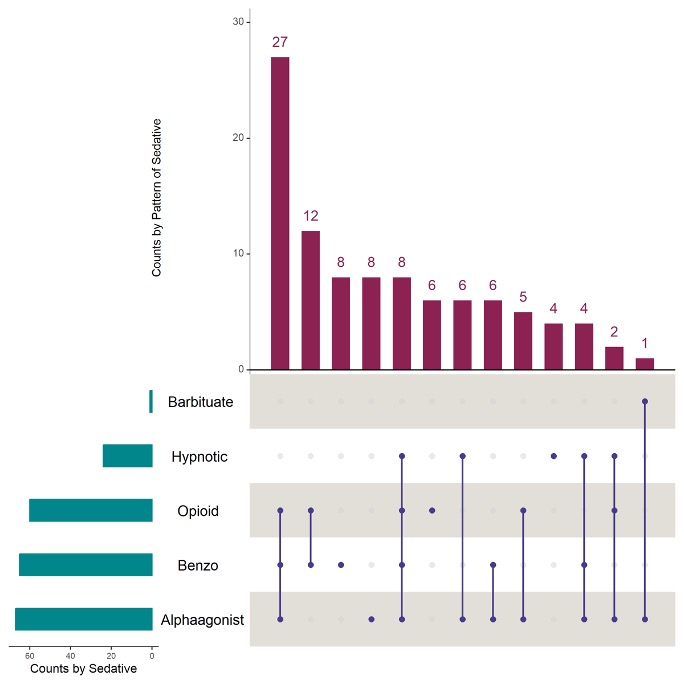 The horizontal green bars at the bottom of the graph represent the number of patients receiving medications from each drug class. The vertical red bars represent the numbers of infants receiving each combination of medications, with blue bars below depicting each combination of medication exposures.
The horizontal green bars at the bottom of the graph represent the number of patients receiving medications from each drug class. The vertical red bars represent the numbers of infants receiving each combination of medications, with blue bars below depicting each combination of medication exposures.