
Neonatal Neurology 1
Session: Neonatal Neurology 1

Jasmeka McCord, MD
Fellow Physician
Emory University School of Medicine
Sunrise, Florida, United States
.png) Abbreviations: SD, standard deviation, kg, kilogram; SIP; spontaneous intestinal perforation.
Abbreviations: SD, standard deviation, kg, kilogram; SIP; spontaneous intestinal perforation.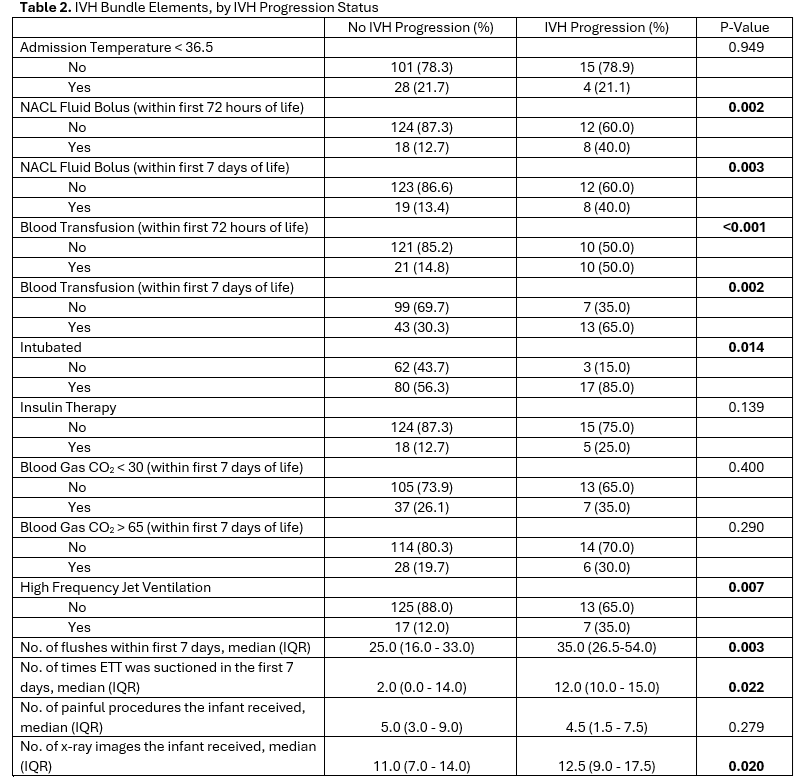 Abbreviations: NACL, sodium chloride; CO2, carbon dioxide; ETT, endotracheal tube; No., number; IQR, interquartile range.
Abbreviations: NACL, sodium chloride; CO2, carbon dioxide; ETT, endotracheal tube; No., number; IQR, interquartile range.